
- Safety & Recalls
- Regulatory Updates
- Drug Coverage
- COPD
- Cardiovascular
- Obstetrics-Gynecology & Women's Health
- Ophthalmology
- Clinical Pharmacology
- Pediatrics
- Urology
- Pharmacy
- Idiopathic Pulmonary Fibrosis
- Diabetes and Endocrinology
- Allergy, Immunology, and ENT
- Musculoskeletal/Rheumatology
- Respiratory
- Psychiatry and Behavioral Health
- Dermatology
- Oncology
BLOG: The goal of vaccines: It’s worth a shot
When vaccines eradicate illnesses (eg, smallpox), life is grand. However, when eradication is impossible (eg, pneumococcus), what is the goal of vaccination? The most essential vaccine function is to reduce the number and/or severity of infections.



Dr HarperWhen vaccines eradicate illnesses (eg, smallpox), life is grand. However, when eradication is impossible (eg, pneumococcus), what is the goal of vaccination? The most essential vaccine function is to reduce the number and/or severity of infections.
Immunity is a screwy thing… a delicate balance between recognizing self versus foreign material. Foreign bacteria and viruses evoke production of antibodies following exposure to antigens. (Does foreign Strep pneumo have a French or an Italian accent?) When microbes and components are packaged up into vaccines, a myriad of circumstances can impact how immunity occurs post vaccination. Those circumstances include the vaccine components, dose, and route as well as the recipient’s age, comorbidities, and other exogenous factors such as diet, stress, smoking status, and even geographical location.1,2
There are 17 vaccine preventable illnesses in the United States:1
- Diphtheria
- Haemophilus influenzae type B
- Hepatitis A
- Hepatitis B
- Human papillomavirus (HPV)
- Influenza
- Measles
- Meningococcal disease
- Mumps
- Pertussis
- Pneumococcal disease
- Poliomyelitis
- Rotavirus
- Rubella
- Tetanus
- Varicella (chickenpox and shingles)
All of the above are reported to the Centers for Disease Control and Prevention (CDC) and then shared via the MMWR as “notifiable diseases” in the United States except HPV, influenza, and rotavirus.3 Comparing historical versus current data demonstrates an impressive vaccine impact (see Graph and Table). Estimated historical annual averages are based from an article published in JAMA in 2007 and range from the early 1900s through the 1990s (typically based on the incidence of disease in the years prior to vaccine introduction).4

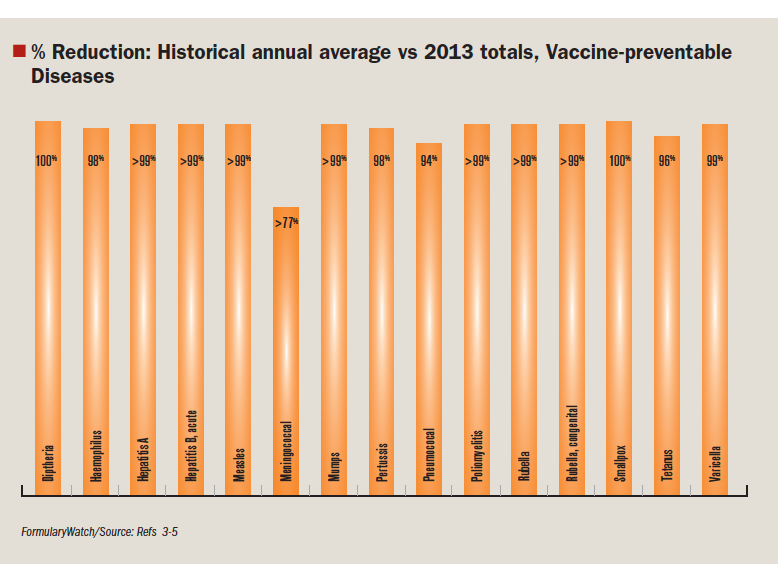
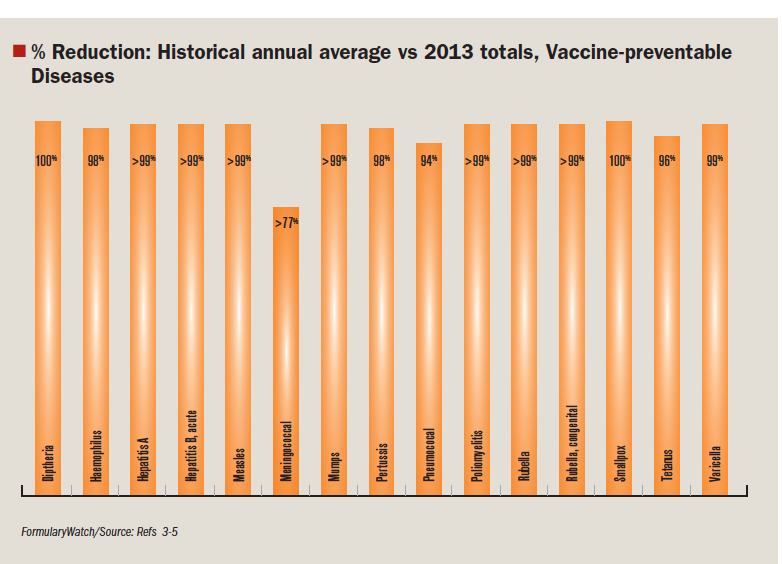
FormularyWatch/Source: Refs 4,5
As evidenced in the Table, not every vaccine-preventable disease is always preventable. These reported cases could be unvaccinated individuals (for whatever reason), but there are also plenty of individuals who have been vaccinated and still become infected following exposure. Any reasons listed in the beginning of this post could be the source of poor vaccine response (endogenous and exogenous factors). A good example of this is pertussis. Pertussis is increasing from a big list of possible reasons including use of acellular versus whole cell vaccines, loss of protective herd-immunity, difficulty differentiating pertussis from other Bordetella infections, lack of understanding of pertussis pathology, and application of various case definitions.5
Researchers from a county health department in Oregon recently reviewed 624 pertussis cases in patients aged 6 weeks to 18 years identified over a 2-year period (2010–2012).6 The median age was 9 years, 52.5% were female, and 75% of patients initiated antibiotic therapy before 20 days. Over half of the cases (54%) were not immunized or not up to date (NUTD). Forty-six percent were up to date (UTD) with pertussis vaccination recommendations. Nineteen patients (3%) had radiologically confirmed pneumonia, 12 (2%) were hospitalized, 3 developed seizures, and 2 developed acute encephalopathy. There were no deaths.
- Vaccinated (both UTD and NUTD) cases less likely to develop severe illness versus unvaccinated:
- Decreased hospitalization (UTD: OR 0.1, 95% confidence Interval [CI] 0.0–0.6, and NUTD: OR 0.1, 95% CI 0.0–0.9).
- Decreased pneumonia rates (UTD: OR 0.5, 95% CI 0.2–1.4, and NUTD: OR 0.5, 95% CI 0.1–0.7).
- Decreased risk for any severe illness (UTD: OR 0.4, 95% CI 0.2–0.8 and NUTD: OR 0.3, 95% CI 0.1–0.8).
- Vaccinated cases were 5 times less likely to be hospitalized and 2.5 times less likely to develop severe illness compared to unvaccinated cases (after adjusting by age).
- Vaccinated (both UTD and NUTD) cases have a shortened duration of illness versus unvaccinated:
- Stop coughing within 100 days (UTD and NUTD, P<0.01). Vaccinations will not always prevent disease.
However, there is evidence to support that disease in the face of partial or complete immunity will mitigate the severity of illness. Wash your hands and vaccinate appropriately.
References
1. Centers for Disease Control and Prevention. Epidemiology and Prevention of Vaccine-Preventable Diseases. Atkinson W, Wolfe S, Hamborsky J, eds. 12th ed. Washington DC: Public Health Foundation, 2012.
2. Van Loveren H, Van Amsterdam JG, Vandebriel RJ, et al. Vaccine-induced antibody responses as parameters of the influence of endogenous and environmental factors. Environ Health Perspect. 2001;109(8):757–764.
3. CDC. Notifiable Diseases and Mortality Tables. MMWR. 2014;63(11):ND-142. http://www.cdc.gov/mmwr/pdf/wk/mm6311md.pdf. Accessed April 3, 2014.
4. Roush SW, Murphy TV; Vaccine-Preventable Disease Table Working Group. Historical comparisons of morbidity and mortality for vaccine-preventable diseases in the United States. JAMA.2007;298(18):2155–2163.
5. Cherry JD. Why do pertussis vaccines fail? Pediatrics. 2012;129(5):968–970.
6. Barlow RS, Reynolds LE, Cieslak PR, et al. Vaccinated children and adolescents with pertussis infections have decreased illness severity and duration, Oregon 2010-2012. Clin Infect Dis.2014 Mar 14. [Epub ahead of print]
Dr Harper graduated from the University of Florida with her doctor of pharmacy and then went on to complete a pharmacy residency at Buffalo General Hospital in Buffalo, N.Y. She then became a clinical coordinator/clinical manager at Millard Fillmore Gates in Buffalo, NY; Roosevelt Hospital in New York City, N.Y.; Chippenham Hospital in Richmond, Va.; and Vail Valley Medical Center in Vail, Colo., before coming to Poudre Valley Hospital in 2007. In addition to being the clinical coordinator at Poudre Valley Hospital, she also is the residency program director for post graduate year-1 pharmacists.




FDA Issues Complete Response Letter for Pz-Cel to Treat Epidermolysis Bullosa
April 22nd 2024Prademagene zamikeracel is a cell therapy designed to incorporate the functional collagen-producing COL7A1 gene into a patient’s own skin cells. The FDA is asking for additional information on manufacturing practices.




