
- Safety & Recalls
- Regulatory Updates
- Drug Coverage
- COPD
- Cardiovascular
- Obstetrics-Gynecology & Women's Health
- Ophthalmology
- Clinical Pharmacology
- Pediatrics
- Urology
- Pharmacy
- Idiopathic Pulmonary Fibrosis
- Diabetes and Endocrinology
- Allergy, Immunology, and ENT
- Musculoskeletal/Rheumatology
- Respiratory
- Psychiatry and Behavioral Health
- Dermatology
- Oncology
Carflizomib: A second-generation proteasome inhibitor for the treatment of myeloma
The introduction of the immunomodulatory drugs and bortezomib, a proteasome inhibitor, has dramatically improved outcomes in patients with relapsed or refractory multiple myeloma.
Abstract
The introduction of the immunomodulatory drugs and bortezomib, a proteasome inhibitor, has dramatically improved outcomes in patients with relapsed or refractory multiple myeloma. The disease remains incurable, however, and several novel agents are currently in development to address this unmet clinical need. Carfilzomib, a second-generation proteasome inhibitor, has demonstrated substantial single-agent activity in heavily pretreated patients in several phase 2 trials. The overall response rate in the pivotal phase 2b study was 24%, and median duration of response was 7.4 months. Carfilzomib was well tolerated, with only 12% of patients discontinuing treatment due to adverse events. More importantly, no peripheral neuropathy was observed, even in subjects with baseline symptoms. Carfilzomib was granted accelerated approval by FDA on July 20, 2012, for the treatment of patients with multiple myeloma who have received at least 2 prior therapies. The approval is based on response rate; no results are available, at this time, that demonstrate a clinical benefit, such as improvement progression-free survival or overall survival. Ongoing clinical trials are also evaluating carfilzomib's activity in the first-line setting in multiple myeloma and its safety and efficacy in advanced solid tumors. (Formulary. 2012; 47:282–286, 308.)
Although multiple myeloma (MM) only accounts for 1% of overall cancers, it is the second most prevalent blood cancer after non-Hodgkin lymphoma. The American Cancer Society has estimated that in 2012, 21,700 new cases of MM will be diagnosed in the United States, including 12,190 cases in men and 9,500 cases in women, and MM will cause an estimated 10,710 deaths.1
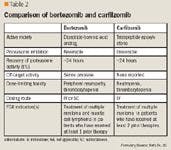
Protein degradation pathway is one of the emerging targets in the treatment of several cancers, including MM. The ubiquitin-proteasome pathway plays a major role in the maintenance of protein homeostasis and the degradation of many proteins involved in cell cycle, proliferation, and apoptosis. Proteasome inhibition in malignant cells leads to accumulation of target proteins followed by induction of cell death.3 After demonstrating single-agent efficacy in the treatment of relapsed and refractory disease, bortezomib was the first proteasome inhibitor approved for the treatment of MM. However, bortezomib therapy has several limitations, as adverse effects include painful peripheral neuropathy (PN), thrombocytopenia, and emergence of secondary resistance.
Carfilzomib (PR-171, Kyprolis) is a second-generation proteasome inhibitor being evaluated for treatment of relapsed and/or refractory MM as well as for first-line therapy in patients with newly diagnosed disease. In July 2012, FDA granted accelerated approval to carfilzomib for the treatment of patients with multiple myeloma who have received at least 2 prior therapies, including bortezomib and an immunomodulatory agent, and have demonstrated disease progression on or within 60 days of the completion of the last therapy. The approval was based on an open-label, single-arm, phase 2b trial evaluating 266 heavily pretreated patients. Carfilzomib is being evaluated in 2 pivotal phase 3 trials, Carfilzomib for Advanced Refractory Multiple Myeloma European Study (FOCUS) and Carfilzomib, Lenalidomide, and Dexamethasone versus Lenalidomide and Dexamethasone for the Treatment of Patients with Relapsed Multiple Myeloma (ASPIRE).
CHEMISTRY AND PHARMACOLOGY

Carfilzomib is a highly selective inhibitor of chymotrypsin-like (β5) subunit activity of the 20S proteasome and has minimal cross-reactivity with other protease classes. It induces dose- and time-dependent inhibition in vitro and in vivo.6 Proteasome inhibitions results in the accumulation of polyubiquitinated proteins and induction of apoptosis through activation of both the intrinsic and extrinsic caspases' pathways. Carfilzomib induces apoptosis and growth cell cycle arrest in a variety of hematologic and solid tumor cell lines, including MM, acute myeloid leukemia, Burkitt lymphoma, Waldenstrom macroglobulinemia, pancreatic cancer, and lung cancer.7-9
Activity of carfilzomib is enhanced with coadministration of histone deacetylase inhibitors. Vorinostat increases the activity of carfilzomib in diffuse large B-cell lymphoma cells resistant or sensitive to bortezomib via increased mitochondrial injury, caspase activation, apoptosis through Jun NH2-terminal kinase, and p38 mitogen-associated protein kinase activation.10,11
Treatment with carfilzomib can overcome primary and secondary resistance to bortezomib and several chemotherapeutic agents in cell lines and in patient-derived clinical samples.12 However, carfilzomib resistance in cell lines, likely caused by P glycoprotein upregulation and multi-drug resistance-related efflux pumps, has been observed. Resistance can be overcome in vitro with the addition of the P-glycoprotein inhibitor verapamil, or by addition of peptide analogs lacking the pharmacophore.13
PHARMACOKINETICS
Preclinical pharmacokinetic (PK) properties of carfilzomib were evaluated in rats and monkeys. After a single intravenously administered dose, the drug was rapidly eliminated from plasma, with a terminal half-life in rats and monkeys of 15 and 7.2 minutes, respectively. Prolonged dose-dependent inhibition of proteasome activities was observed in all tissues except the brain, an indication that the drug does not cross the blood-brain barrier.14

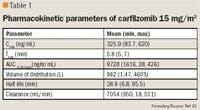
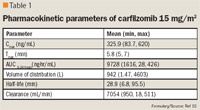
The PK profile of carfilzomib does not seem to be affected by renal impairment. The PK parameters in patients with mild renal impairment (creatinine clearance, 50–79 mL/min); moderate renal impairment (creatinine clearance, 30–49 mL/min); and severe renal impairment (creatinine clearance, <30 mL/min) were similar to those in patients with normal renal function.16
CLINICAL TRIALS
Carfilzomib is under evaluation for use in treatment of MM and some solid tumors. The NDA for carfilzomib for treatment of patients with relapsed or refractory MM was supported by efficacy data from 526 patients enrolled in 4 phase 2 studies and safety data from 768 patients enrolled in phase 1 and phase 2 studies.
The pivotal study, PX-171-003A1, was an open-label, single-arm, phase 2b study, in which carfilzomib showed significant, durable responses in patients with relapsed or refractory MM who were previously treated with at least 2 therapies (bortezomib and either thalidomide or lenalidomide; and an alkylator and/or anthracycline).17–19 Carfilzomib was administered intravenously at 20 mg/m2 on days 1, 2, 8, 9, 15, and 16 of a 28-day cycle for 12 cycles. After cycle 1, the dose was increased to 27 mg/m2. The trial included 266 patients, of which 257 had responses evaluated. These patients were heavily pretreated: the mean number of prior therapies was 5.4, 74% of patients had been treated with autologous transplantation, and the majority of patients (95%) were judged refractory to their most recent therapy. An independent review committee assessed responses based on the International Myeloma Working Group criteria. The overall response rate (ORR) was 24% with median duration of response (DOR) of 7.4 months (95% confidence interval [CI], 6.2–10.3). Cytogenetic studies were available for 229 patients, and 71 of the 229 had at least one cytogenetic abnormality.18 Patients with unfavorable cytogenetic characteristics had an ORR of 28% and DOR of 7 months (95% CI, 4–10).18 The median overall survival rate was 15.5 months (95% CI, 12.7–19.0).18 The clinical benefit response (ORR + minimal response) was 36%.17 The drug was well tolerated, and hematologic adverse events were the most common complications. Grade 3 or higher adverse events were thrombocytopenia (22%), anemia (20%), lymphopenia (10%), pneumonia (8%), neutropenia (8%), fatigue (7%), hyponatremia (5%), and hypercalcemia (5%).17 Seventy-seven percent of patients with baseline grade 1 or 2 PN tolerated therapy without worsening of symptoms or decreased response (ORR, 24%).17 Less than 1% of patients had new-onset grade 3 or higher PN.17,19
The second open-label, multicenter, phase 2 study, PX-171-004, enrolled less heavily pretreated patients compared with PX-171-003A1.20 One hundred twenty-nine bortezomib-naïve and 35 bortezomib-treated patients with relapsed or refractory MM were enrolled. Patients had to have been treated with 1 to 3 regimens previously. Cohort 1 (n=59) was administered carfilzomib 20 mg/m2 intravenously on days 1, 2, 8, 9, 15, 16 of a 28-day cycle. Cohort 2 (n=70) was administered carfilzomib 20 mg/m2 intravenously for cycle 1, which was escalated to 27 mg/m2 for all subsequent cycles, for 12 cycles. An independent review committee assessed responses based on the International Myeloma Working Group criteria. The ORR in cohort 1 was 42.4%, and the ORR in cohort 2 was 52.2%. The median DOR in cohort 1 was 13.1 months and was not reached in cohort 2. The median time to progression was 8.3 months in cohort 1 and was not reached in cohort 2. Complete response was achieved in 2 patients (3.4%) in cohort 1 and 1 patient (1.5%) in cohort 2. Clinical benefit response rates were 59.3% and 64.2% in cohorts 1 and 2, respectively. As in PX-171-003A1, grade 3 toxicities were mostly hematologic and included lymphopenia (16.3%), anemia (14.7%), neutropenia (13.2%), thrombocytopenia (13.2%), and pneumonia (12.4%). The most common adverse events overall were fatigue (62.0%), nausea (48.8%), anemia (41.9%), dyspnea (38.8%), cough (34.1%), and pyrexia (34.1%). The overall incidence of treatment-emergent PN was 17.1% (1 patient with grade 3 PN; no patients with grade 4 PN).20
Carfilzomib showed promising activity in the first-line setting in combination with lenalidomide and low-dose dexamethasone (CRd) in patients with newly diagnosed MM in a phase 1/2 trial.21 Patients had to have measureable disease and be symptomatic. Grade 3/4 neuropathy at baseline excluded enrollment in the study. Patients received CRd every 28 days for a maximum of 8 cycles until disease progression, or until they experienced unacceptable toxicity. After 8 cycles, patients received maintenance CRd for a total of 24 cycles followed by off-protocol single-agent lenalidomide. Carfilzomib was given at 20, 27, or 36 mg/m2 on days 1, 2, 8, 9, 15, and 16 and on days 1, 2, 15, 16 after cycle 8. Lenalidomide 25 mg was given on days 1 through 21. Weekly doses of dexamethasone 40 mg were administered during cycles 1 through 4 and 20 mg from cycle 5 onward. After cycle 4, patients who were eligible for stem cell transplantation were able to undergo cell collection and then proceed with transplantation or resume CRd treatment. The trial included 53 patients from 4 sites. The median treatment duration was 12 cycles, and a single patient discontinued treatment during induction for CRd toxicity. Sixty-two percent of patients achieved near-complete response (nCR), and 98% of patients had at least partial response (PR). Thirty-six patients received 8 or more cycles with nCR rate of 78%. The 24-month progression-free survival estimate was 92% during a median 13-month follow up. A 20% dose-limiting toxicity (DLT) cutoff was used to determine the maximum tolerable dose. The probability of a DLT shows a trend of increasing with increasing dose: 5.9% at 20 mg/m2, 8.1% at 27 mg/m2, and 12% at 36 mg/m2. During phase 2, the 36 mg/m2 carfilzomib dose was used, as the 20% DLT probability was not achieved. Grade 3/4 adverse events during cycles 1 through 8 included hypophosphatemia (25%), hyperglycemia (23%), anemia (21%), thrombocytopenia (17%), and neutropenia (17%). Twenty-three percent of patients experienced grade 1/2 PN. During maintenance CRd, the most common toxicities were lymphopenia (30%), leucopenia (26%), and fatigue (25%).21
The safety and PK of carfilzomib were also evaluated in patients with relapsed and refractory MM and baseline renal impairment, including patients receiving hemodialysis (see PK discussion).
Carfilzomib is under evaluation in 2 phase 3 trials. The ASPIRE trial analyzes the safety and efficacy of carfilzomib for treatment of MM relapse in combination with lenalidomide and CRd versus lenalidomide and CRd alone. The primary end point is progression-free survival. The FOCUS trial assesses the role of single-agent carfilzomib compared with corticosteroid agent with or without oral cyclophosphamide in relapsed and refractory MM for European approval of carfilzomib. The primary end point is overall survival.
ADVERSE EVENTS
Carfilzomib is generally well tolerated, and treatment-related adverse events are mainly low grade in severity. Safety data are available from 526 patients enrolled in all phase 2 trials and 266 patients enrolled in phase 3 trials. Progression of disease was the most common cause of death (33 of 792 patients; 4%). Less than 2% of patients died due to cardiac, hepatic, or pulmonary causes. The most common serious adverse events in patients enrolled in phase 2 trials were cardiac disorders (8%), respiratory disorders (7%), and hepatobiliary disorders (<1%). The most common serious adverse events in patients enrolled in phase 3 trials were infections and infestations (7%), cardiac disorders (4%) and respiratory disorders (4%). Common adverse events noted in the phase 2 trials (>20%) were fatigue, anemia, nausea, thrombocytopenia, dyspnea, diarrhea, pyrexia, headache, upper respiratory tract infection, cough, lymphemia, blood creatinine increase, peripheral edema, vomiting, neutropenia, constipation, and back pain. Grade 3 or higher adverse events were mostly hematologic and included thrombocytopenia, anemia, and lymphopenia. The most common reasons patients discontinued therapy in phase 2 trials were cardiac disorders (6%) and respiratory disorders (4%). PN, a dose-limiting adverse event with bortezomib, was minimally noted with carfilzomib. Grade 3 PN occurred in less than 1% of patients, and no patients had dose adjustments or discontinuation due to PN. Patients with baseline PN tolerated therapy well without worsening of symptoms.18–21
DRUG INTERACTIONS
Carfilzomib is excreted primarily as inactive metabolites derived from peptide and epoxide hydrolysis, and it has no reported drug interactions.22 Although carfilzomib has been shown to be a moderate cytochrome P (CYP)3A4 inhibitor in vitro, it had no effect on the the PK of midazolam, a CYP3A probe, in a drug interaction study conducted in cancer patients.
In vitro studies using human hepatocytes have also shown that carfilzomib does not induce CYP3A4 and 1A2. These studies indicate that carfilzomib is unlikely to have any interactions or clinically relevant effects on the disposition of drugs metabolized by the CYP enzyme system.14
DOSING AND ADMINISTRATION
Carfilzomib is administered intravenously at 20 mg/m2 over 2 to 10 minutes on days 1, 2, 8, 9, 15, and 16 in cycle 1, with escalation to 27 mg/m2 in subsequent cycles as tolerated every 28 days. The dose should be based on patient's actual body surface area at baseline up to a maximum of 2.2 m2. The dose should be recalculated for a weight change of ≥ 20% and treatment may be continued until disease progression or unacceptable toxicity. Infusion-related reactions or "first-dose effect" have been reported in early clinical trials. To reduce these reactions, which include shortness of breath, hypotension, and angina during or shortly after the infusion, dexamethasone (4 mg orally or intravenously) should be administered before each dose administration in the first 2 cycles and thereafter, if infusion reaction symptoms develop or reappear. Fluids, 250 to 500 mL, should also be administered intravenously before and after each dose in cycle 1 and as needed in subsequent cycles to reduce the risk of renal toxicity and tumor lysis syndrome. No dose adjustment is recommended based on age, sex, race, or baseline renal impairment. While carfilzomib exposure is unlikely to be affected by hepatic impairment due to its extrahepatic metabolism, patients with ALT/AST ≥ 3 × upper limit of normal (ULN) and bilirubin ≥ 2 × ULN were excluded from the clinical trials and specific dosing recommendations for these patients are not available.
Dose modification guidelines for hematologic and non-hematologic toxicity during treatment are included in the drug product information.
FORMULARY CONSIDERATIONS
Carfilzomib demonstrated significant activity in relapsed and/or refractory myeloma, and it has one of the highest single-agent response rates (up to 52% in patients who had never received bortezomib) and longest durations of responses observed in this patient population. However, data on its impact on progression-free survival or overall survival are currently not available.

Carfilzomib will be an effective treatment option in patients who are either intolerant or resistant to bortezomib. Ongoing clinical trials will further define its role in the first-line setting, its safety and efficacy in patients with other malignancies, and early markers for best myeloma response.26 These studies will also determine whether the activity seen in the pivotal phase study was enhanced by the addition of low dose dexamethasone, an active agent in MM at higher doses, to prevent infusion-related toxicities.
Carfilzomib joined bortezomib as the only FDA-approved proteasome inhibitors. However, the market may soon be crowded with several other inhibitors in various stages of clinical development, including orally active agents. Efficacy, resistance data, adverse-effect profile, and patient convenience should be evaluated carefully before a formulary agent is chosen.
Dr Adib is oncology clinical pharmacist, Yale New Haven Hospital, New Haven, CT. Dr Patel is oncology clinical pharmacist, Yale New Haven Hospital, New Haven, CT. Dr Abdelghany is coordinator, Investigational Drug Service, Yale New Haven Hospital, New Haven, CT.
Disclosure Information: The authors report no financial disclosures as related to products discussed in this article.
In each issue, the "Focus on" feature reviews a newly approved or investigational drug of interest to pharmacy and therapeutics committee members. The column is coordinated by Robert A. Quercia, MS, RPh, medical editor, University of Connecticut/Hartford Hospital, Evidence-based Practice Center, Hartford, Conn., and adjunct associate professor, University of Connecticut School of Pharmacy, Storrs, Conn; and by Craig I. Coleman, PharmD, associate professor of pharmacy practice, University of Connecticut School of Pharmacy, and director, Pharmacoeconomics and Outcomes Studies Group, Hartford Hospital.
EDITORS' NOTE: The clinical information provided in "Focus on" articles is as current as possible. Due to regularly emerging data on developmental or newly approved drug therapies, articles include information published or presented and available to the author up until the time of the manuscript submission.
REFERENCES
1. American Cancer Society. Multiple myeloma. January 17, 2012. Available at http://www.cancer.org/Cancer/MultipleMyeloma/DetailedGuide/multiple-myeloma-key-statistics. Accessed July 12, 2012.
2. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: multiple myeloma. Version.1.2012. Available at http://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf. Accessed May 20, 2012
3. Glickman MH, Ciechanover A. The ubiquitin-proteasome proteolytic pathway: destruction for the sake of construction. Physiol Rev. 2002; 82(2):373–428.
4. Screen M, Britton M, Downey SL, et al. Nature of pharmacophore influences active site specificity of proteasome inhibitors. J Biol Chem. 2010; 285(51):40125–40134.
5. Kuhn DJ, Orlowski RZ, Bjorklund CC. Second generation proteasome inhibitors: carfilzomib and immunoproteasome-specific inhibitors (IPSIs). Curr Cancer Drug Targets. 2011; 11(3):285–295.
6. Parlati F, Lee SJ, Aujay M, et al. Carfilzomib can induce tumor cell death through selective inhibition of the chymotrypsin-like activity of the proteasome. Blood. 2009; 114(16):3439–3447.
7. Demo SD, Kirk CJ, Aujay MA, et al. Antitumor activity of PR-171, a novel irreversible inhibitor of the proteasome. Cancer Res. 2007; 67(13):6383–6391.
8. Sacco A, Aujay M, Morgan B, et al. Carfilzomib-dependent selective inhibition of the chymotrypsin-like activity of the proteasome leads to antitumor activity in Waldenstrom's macroglobulinemia. Clin Cancer Res. 2011; 17(7):1753–1764.
9. Stapnes C, Doskeland AP, Hatfield K et al. The proteasome inhibitors bortezomib and PR-171 have antiproliferative and proapoptotic effects on primary human acute myeloid leukaemia cells. Br J Haem. 2007; 136:814–828.
10. Dasmahapatra1 G, Lembersky D, Kramer L, et al. The pan-HDAC inhibitor vorinostat potentiates the activity of the proteasome inhibitor carfilzomib in human DLBCL cells in vitro and in vivo. Blood. 2010; 115(22):4478–4487.
11. Dasmahapatra G, Lembersky D, Son MP, et al. Carfilzomib interacts synergistically with histone deacetylase inhibitors in mantle cell lymphoma cells in vitro and in vivo. Mol Cancer Ther. 2011; 10(9):1686–1697.
12. Kuhn DJ, Chen Q, Voorhees PM, et al. Potent activity of carfilzomib, a novel, irreversible inhibitor of the ubiquitin-proteasome pathway, against preclinical models of multiple myeloma. Blood. 2007; 110(9):3281–3290.
13. Ao L, Wu Y, Kim D, et al. Development of peptide-based reversing agents for P-glycoprotein-mediated resistance to carfilzomib. Mol Pharm. 2012 June 16 [epub ahead of print].
14. Yang J, Wang Z, Fang Y, et al. Pharmacokinetics, pharmacodynamics, metabolism, distribution, and excretion of carfilzomib in rats. Drug Metab Dispos. 2011; 39(10):1873–1882.
15. O'Connor OA, Stewart AK, Vallone M, et al. A phase 1 dose escalation study of the safety and pharmacokinetics of the novel proteasome inhibitor carfilzomib (PR-171) in patients with hematologic malignancies. Clin Cancer Res. 2009; 15(22):7085–7091.
16. Jain S, Diefenbach C, Zain J, O'Connor OA. Emerging role of carfilzomib in treatment of relapsed and refractory lymphoid neoplasms and multiple myeloma. Core Evid. 2011; 6:43–57.
17. Siegel D, Martin T, Wang M, et al. Results of PX-171-003-A1, an open-label, single-arm, phase 2 (Ph 2) study of carfilzomib (CFZ) in patients (pts) with relapsed and refractory multiple myeloma (MM) [ASH Annual Meeting abstract]. Blood. 2010; 116:abstract 985.
18. Siegel D, Martin T, Wang M, et al: PX-171-003-A1, an open-label, single-arm, phase (Ph) II study of carfilzomib (CFZ) in patients (pts) with relapsed and refractory multiple myeloma (R/R MM): Long-term follow-up and subgroup analysis [abstract]. J Clin Oncol. 2011; 29 (suppl) abstract 8027.
19. Onyx Pharmaceuticals Inc. Briefing document, Oncologic Drugs Advisory Committee, NDA 202714: carfilzomib (Kyprolis). Available at http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee/UCM308565.pdf. Accessed July 12, 2012.
20. Vij R, Wang M, Kaufman JL, et al. An open-label, single-arm, phase 2 (PX-171-004) study of single-agent carfilzomib in bortezomib-naïve patients with relapsed and/or refractory multiple myeloma. Blood. 2012; 119(24):5661–5670.
21. Jakubowiak AJ, Dytfeld D, Griffith KA, et al. A phase 1/2 study of carfilzomib in combination with lenalidomide and low-dose dexamethasone as a frontline treatment for multiple myeloma. Blood. 2012 Jun 4 [epub ahead of print].
22. Khan ML, Stewart AK. Carfilzomib: a novel second-generation proteasome inhibitor. Future Oncol. 2011; 7(5):607–612
23. Arastu-Kapur S, Anderl JL, Kraus M, et al. Nonproteasomal targets of the proteasome inhibitors bortezomib and carfilzomib: a link to clinical adverse events. Clin Cancer Res. 2011; 17(9):2734–2743.
24. Velcade [prescribing information]. Cambridge, MA: Mellenium Pharmaceuticals; 2012.
25. Moreau P. The future of therapy for relapsed/refractory multiple myeloma: emerging agents and novel treatment strategies. Semin Hematol. 2012; 49 (suppl 1):S33–S46.
26. Zangari M, Aujay M, Zhan F, et al. Alkaline phosphatase variation during carfilzomib treatment is associated with best response in multiple myeloma patients. Eur J Haematol. 2011; 86(6):484–487.


Coalition promotes important acetaminophen dosing reminders
November 18th 2014It may come as a surprise that each year Americans catch approximately 1 billion colds, and the Centers for Disease Control and Prevention estimates that as many as 20% get the flu. This cold and flu season, 7 in 10 patients will reach for an over-the-counter (OTC) medicine to treat their coughs, stuffy noses, and sniffles. It’s an important time of the year to remind patients to double check their medicine labels so they don’t double up on medicines containing acetaminophen.
Support consumer access to specialty medications through value-based insurance design
June 30th 2014The driving force behind consumer cost-sharing provisions for specialty medications is the acquisition cost and not clinical value. This appears to be true for almost all public and private health plans, says a new report from researchers at the University of Michigan Center for Value-Based Insurance Design (V-BID Center) and the National Pharmaceutical Council (NPC).
Management of antipsychotic medication polypharmacy
June 13th 2013Within our healthcare-driven society, the increase in the identification and diagnosis of mental illnesses has led to a proportional increase in the prescribing of psychotropic medications. The prevalence of mental illnesses and subsequent treatment approaches may employ monotherapy as first-line treatment, but in many cases the use of combination of therapy can occur, leading to polypharmacy.1 Polypharmacy can be defined in several ways but it generally recognized as the use of multiple medications by one patient and the most common definition is the concurrent use of five more medications. The presence of polyharmacy has the potential to contribute to non-compliance, drug-drug interactions, medication errors, adverse events, or poor quality of life.
Medical innovation improves outcomes
June 12th 2013I have been diagnosed with stage 4 cancer of the pancreas, a disease that’s long been considered not just incurable, but almost impossible to treat-a recalcitrant disease that some practitioners feel has given oncology a bad name. I was told my life would be measured in weeks.

