
- Safety & Recalls
- Regulatory Updates
- Drug Coverage
- COPD
- Cardiovascular
- Obstetrics-Gynecology & Women's Health
- Ophthalmology
- Clinical Pharmacology
- Pediatrics
- Urology
- Pharmacy
- Idiopathic Pulmonary Fibrosis
- Diabetes and Endocrinology
- Allergy, Immunology, and ENT
- Musculoskeletal/Rheumatology
- Respiratory
- Psychiatry and Behavioral Health
- Dermatology
- Oncology
Ceftobiprole: The first anti-MRSA cephalosporin antibiotic
Ceftobiprole is the first anti-MRSA cephalosporin antibiotic to be sumbitted to FDA for approval. If approved, the drug will likely be considered a second-line antibiotic for the treatment of cSSSIs.



Key Points
• Abstract
Serious infections caused by resistant gram-positive cocci continue to increase in prevalence and significance. An NDA for ceftobiprole, an investigational novel broad-spectrum cephalosporin antibiotic, was submitted on May 18, 2007, for the treatment of complicated skin and skin-structure infections (cSSSIs), including diabetic foot infections. Ceftobiprole has demonstrated in vitro and in vivo activity against methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-intermediate S aureus (VISA), vancomycin-resistant S aureus (VRSA), multidrug-resistant Streptococcus pneumoniae, Enterococcus faecalis, and some gram-negative bacteria, including Enterobacteriaceae that do not produce extended-spectrum beta-lactamases (ESBLs) and ceftazidime/cefepime-susceptible Pseudomonas aeruginosa. In clinical trials, ceftobiprole has demonstrated noninferiority to vancomycin monotherapy and vancomycin plus ceftazidime for the treatment of cSSSIs. Phase 3 clinical trials have also been conducted to assess ceftobiprole's efficacy in the treatment of community- and hospital-acquired pneumonia; full results have not yet been released. Ceftobiprole was well tolerated in clinical trials, with patients experiencing only mild adverse events (most commonly a caramel taste alteration after administration). If approved, ceftobiprole's in vitro activity against resistant gram-positive bacteria, particularly MRSA, combined with its demonstrated clinical efficacy for the treatment of cSSSIs and its mild adverse-event profile, will likely make the drug an attractive addition to the antimicrobial armamentarium. (Formulary. 2008;43:66–78.)
The increasing prevalence of resistance among clinically significant pathogens to current antimicrobial agents is a worldwide concern. Gram-positive cocci, in particular, are responsible for many severe infections in community and hospital settings; and the multidrug resistance of these organisms is alarming because this resistance compromises therapeutic options.
Although MRSA has long been considered a hospital-acquired pathogen, it is now present outside the hospital setting, in the community. Strains of community-acquired MRSA (CA-MRSA) differ from nosocomial strains in that they demonstrate greater susceptibility to non-beta-lactam antibiotics but are more virulent, in part because of the presence of the gene encoding Panton-Valentine leukocidin (PVL), a toxin responsible for the release of neutrophil chemotactic factors and for subsequent inflammation and tissue destruction.1,2 A recent study demonstrated that at 11 emergency departments (EDs) across the United States, CA-MRSA was the most common cause of complicated skin and skin-structure infections (cSSSIs) among patients who presented to the ED.3 The high prevalence of MRSA in hospital settings as well as the media's recent focus on CA-MRSA as the new "superbug" has caused prescribers to request more treatment options for this pathogen. Nonhospitalized patients with cSSSIs usually successfully respond to a variety of oral antibiotics, including older agents (eg, trimethoprim/sulfamethoxazole, doxycycline, and clindamycin, which are not FDA approved to treat cSSSIs) and newer drugs such as oral linezolid, which is reserved for patients who cannot tolerate older agents or who have infection relapses. Patients with more severe infections may require hospitalization and intravenous (IV) antibiotic therapy. Vancomycin is considered by many to be the gold standard for the treatment of MRSA infections in the hospital setting; however, its widespread use has led to the emergence of strains with increasing minimum inhibitory concentrations (MICs) and, on some occasions, clinical resistance. Vancomycin-intermediate S aureus (VISA) (vancomycin MIC=4–8 mcg/mL) and vancomycin-resistant S aureus (VRSA) (vancomycin MIC ≥16 mcg/mL) are rare but have been documented globally and have resulted in poor clinical outcomes in patients with bacteremia.1 Moreover, other gram-positive bacteria such as multidrug-resistant Streptococcus pneumoniae and vancomycin-resistant Enterococcus (VRE) continue to cause serious infections, which also present a therapeutic challenge.
The emerging resistance to vancomycin among gram-positive cocci and the poor tissue penetration and weak antibacterial activity of this glycopeptide, has led researchers to develop novel antistaphylococcal agents. Linezolid, daptomycin, tigecycline, and quinupristin/dalfopristin have been introduced into clinical practice, each with their own clinical pros and cons. Additionally, new lipoglycopeptides (dalbavancin, telavancin, and oritavancin) are also being investigated for the treatment of cSSSIs and other indications.2
Ceftobiprole (Basilea/Johnson & Johnson), a broad-spectrum cephalosporin antibiotic with activity against gram-negative and multiresistant gram-positive bacteria, including MRSA, is among the first of several beta-lactams being developed with targeted activity against the methicillin-resistant phenotype. An NDA for ceftobiprole was submitted on May 18, 2007, for the treatment of cSSSIs, including diabetic foot infections. Initial interest in this compound has been focused on its potential use in the treatment of cSSSIs, as studied in 2 large, phase 3 trials. Additionally, because of this agent's broad-spectrum activity against gram-positive and gram-negative bacteria, ceftobiprole may prove to be an attractive alternative for the treatment of hospital-acquired pneumonia (HAP), a disease in which MRSA is often the most commonly isolated pathogen, followed by various gram-negative Enterobacteriaceae (eg, Escherichia coli, Klebsiella pneumoniae, Enterobacter species) and Pseudomonas aeruginosa. Phase 3 studies of ceftobiprole's efficacy in the treatment of nosocomial pneumonia have also recently been completed.4
CHEMISTRY AND PHARMACOLOGY
Ceftobiprole (formerly known as BAL9141) is the active component of the prodrug ceftobiprole medocaril (formerly known as BAL5788). It is a pyrrolidinone-3-ylidenemethyl cephem with a basic C3 side chain.4 Because of this agent's poor solubility at physiologic pH, ceftobiprole is administered as the water-soluble prodrug, which is rapidly and almost completely converted to the active drug plus diacetyl and carbon dioxide by plasma esterases.5 Like all beta-lactam antibiotics, ceftobiprole produces its bactericidal effects by inhibiting cell wall synthesis via prevention of the cross-linking of peptides on the mucosaccharide chains that make up the cell wall. This is accomplished by binding to and inhibiting the penicillin-binding proteins (PBPs). As a result, bacterial cell walls are weakened and susceptible to osmotic pressure and cell lysis.
The broad-spectrum activity of ceftobiprole is due to the inhibition of PBPs in both gram-positive and gram-negative bacteria.5 MRSA contains a supplemental peptidoglycan transpeptidase, PBP2' (PBP-2a), which is different from normal PBPs and is responsible for its methicillin resistance. PBP2' is encoded by the mecA gene that is part of the staphylococcal cassette chromosome (SCCmec) element and interacts with the bacterial cell wall to prevent cell destruction by beta-lactam antibiotics. Although most available beta-lactams don't efficiently inhibit PBP2', ceftobiprole binds tightly to its active site and then forms a stable acyl-enzyme complex that is resistant to hydrolysis.6 In addition, ceftobiprole inhibits PBP2x in penicillin-resistant S pneumoniae as well as PBP3 and other PBPs in certain gram-negative bacteria such as E coli and P aeruginosa.5
PHARMACOKINETICS AND PHARMACODYNAMICS
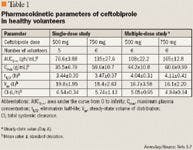
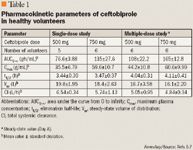
Single and multiple-dose administration studies of ceftobiprole 125 to 1,000 mg have been performed (Table 1).5,7 In one study, the prodrug BAL5788 was rapidly metabolized to ceftobiprole, and no prodrug could be measured in plasma after the end of the infusion.7 In single-dose studies involving healthy volunteers, the peak plasma level was achieved at the end of the 30-minute infusion and following that, a biphasic decrease of ceftobiprole's concentration was observed as the agent was distributed rapidly from the systemic circulation into other tissue compartments. The volume of distribution was estimated to be 15 to 18 L, which is approximately the volume of extracellular fluid. After administration of increasing doses of ceftobiprole, the area under the concentration curve from 0 to infinity (AUC0–∞) and the maximum concentration in plasma (Cmax) exhibited dose-dependent proportionality for all doses. Additionally, the volume of distribution at steady state (Vss) and the total systemic clearance were dose independent.5 After repeated administration of the drug over 8 days, there was no significant accumulation in plasma, and the elimination half-life of ceftobiprole (t1/2) was estimated to be 3 to 4 hours.7 Although gender itself has not been demonstrated to significantly affect ceftobiprole's pharmacokinetics, pharmacokinetic differences have been observed between male and female patients, primarily because of differences in body weight/size.8 Ceftobiprole demonstrates a low percentage of protein binding (16%).9 Its penetration into respiratory tissues is of great importance, as the antibiotic is being studied as a therapeutic option for pneumonia. In murine models, it was demonstrated that the concentration of ceftobiprole in epithelial lining fluid (ELF) increased proportionately with increased doses of the drug. Moreover, concentrations of ceftobiprole in the ELF were greater than those in the whole lung tissue, as the latter contains both intracellular and extracellular fluid.10 In addition, the concentrations of ceftobiprole in the ELF exceeded the MIC of S aureus isolates (60%–94% of the free drug in plasma). The agent's penetration in lung tissue was estimated to be 25% (range, 17%–40%).10

Studies have demonstrated that pharmacokinetic parameters observed in patients with cSSSIs are comparable to those observed in healthy volunteers; however, the pharmacokinetic profile of ceftobiprole in a critically ill patient population has not yet been reported.11
Because beta-lactams demonstrate time-dependent antimicrobial activity, the pharmacodynamic parameter that best correlates with their efficacy is the percent of the dosing interval in which free drug concentrations remain above the MIC (fT>MIC). For cephalosporins in general, values of 35% to 40% fT>MIC and 60% to 70% fT>MIC are required for a bacteriostatic and bactericidal effect, respectively. Two studies in healthy volunteers demonstrated that after the administration of ceftobiprole 500 mg and ceftobiprole 750 mg, the time that the total drug concentration remained above 4 mcg/mL (the MIC at which 100% of MRSA strains are inhibited) was 5 to 7 hours and 7 to 9 hours, respectively, which satisfies the bactericidal exposure requirement when the dosing is administered every 8 hours.5,12
SPECTRUM OF ACTIVITY
Because of its broad-spectrum binding affinities, ceftobiprole is active against a wide range of gram-positive and gram-negative pathogens (Table 2).13–17 Percent susceptibility cannot be defined at this time because susceptibility break points have not been confirmed by FDA. Perhaps ceftobiprole's most interesting characteristic is its activity against S aureus strains, including MRSA. Ceftobiprole has demonstrated activity against isolates of methicillin-susceptible S aureus (MSSA) and against isolates of MRSA.13 The spectrum of activity of ceftobiprole also includes methicillin-susceptible and methicillin-resistant coagulase-negative staphylococci, VISA, and VRSA, including the Michigan and Pennsylvania strains.13 Moreover, ceftobiprole retains activity against both CA-MRSA and hospital-acquired MRSA (HA-MRSA) genotypes.18 The MICs of MRSA that were demonstrated in 1 study were similarly low regardless of the SCCmec type and the resistance to other antimicrobials (MIC50: 0.5 mcg/mL and MIC90: 2 mcg/mL).19 In 1 study, ceftobiprole was demonstrated to be bactericidal in vitro against most strains except for a single VISA isolate; furthermore, resistance did not develop after exposure of pathogens to subinhibitory concentrations of the drug.13 Ceftobiprole is active against S aureus both in broth and after phagocytosis by macrophages, which is attributed to the agent's enhanced activity at an acidic pH.12
Ceftobiprole is also bactericidal against S pneumoniae, an important feature, as penicillin-resistant, cephalosporin-resistant, and macrolide-resistant strains of S pneumoniae have emerged worldwide. In a study that compared the susceptibility of 299 strains of S pneumoniae to beta-lactams, macrolides, and fluoroquinolones, ceftobiprole was demonstrated to have MICs similar to those of carbapenems and lower than those of the other 6 cephalosporins that were included in the study.14 As was observed in the previously mentioned study with staphylococci, resistance was also not observed among streptococci after multiple passages.



The spectrum of activity of ceftobiprole also extends to gram-negative bacteria (Table 2).13–17 Ceftobiprole is a poor substrate for class A and class C penicillinases, which are produced by S aureus and enteric gram-negatives, but it can be hydrolyzed by class B, class D, and extended-spectrum beta-lactamases (ESBL) and carbapenemases.4,21 Ceftobiprole inhibits Haemophilus influenza and Moraxella catarrhalis, including beta-lactamase producers.16 The agent also inhibits E coli, K pneumoniae, Proteus mirabilis, Morganella morganii, Providencia species, Vibrionaceae species, and Neisseria gonorrhoeae.17 Ceftobiprole has greater microbiological potency against Enterobacter cloacae than ceftriaxone and ceftazidime.22 Some ESBL-producing strains of Enterobacteriaceae and most isolates of Proteus vulgaris are resistant to ceftobiprole.17 Ceftobiprole's in vitro potency against P aeruginosa has been demonstrated to be similar to that of ceftazidime and cefepime.23 In one study, 72% of the 741 isolates were inhibited by ceftobiprole at MIC 4 mcg/mL compared with 73% and 68% with ceftazidime at MIC 4 mcg/mL and cefepime at MIC 4 mcg/mL, respectively.23
The susceptibility of anaerobes to ceftobiprole has also been studied. The agent is active against certain gram-positive anaerobes including Propionibacterium acnes, Peptostreptococcus anaerobius, Clostridium innocuum, Finegoldia magna, Porphyromonas asaccharolytica, and most strains of Porphyromonas somerae. Like most cephalosporins, ceftobiprole is not active against species of the Bacteroides fragilis group, Prevotella bivia, or strains of Prevotella melaninogenica.24
CLINICAL TRIALS




Clinical cure rates were similar between patients treated with ceftobiprole (93.3%) and patients treated with vancomycin (93.5%). Microbiological eradication or presumed eradication occurred in 94.2% and 93.5% of the microbiologically evaluable patients in the ceftobiprole and vancomycin groups, respectively. Approximately 80% of the microbiologically evaluable population had infections caused by S aureus; one-third of these isolates were MRSA. In a subanalysis of patients infected with MRSA, there were no significant differences in clinical cure rates between the treatment groups (ceftobiprole, 91.8% vs vancomycin, 90.0%). In patients with PVL-positive MRSA isolates, ceftobiprole was associated with greater cure rates compared with vancomycin (93.1% vs 84.6%), but this difference was not statistically significant. The incidence of serious adverse events and treatment-emergent AEs was comparable between the treatment groups. Although noninferiority was demonstrated in this study, it is worth noting that the vast majority of S aureus isolates in this trial, including MRSA, had vancomycin MICs of 0.5 mcg/mL, which is lower than the MICs for MRSA in most hospitals today. This was likely a result of the large number of CA-MRSA strains observed in the study.
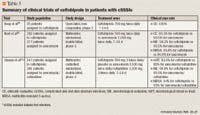
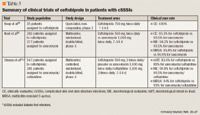
The second phase 3 trial was also a large, randomized, double-blind, multicenter study of ceftobiprole in hospitalized patients with cSSSIs; however, this trial included patients with diabetic foot infections potentially caused by gram-negative pathogens (Table 3).27 The infections were defined as either involving deeper soft tissue or requiring surgical intervention. Patients were also expected to have ≥1 of the following: infection caused by gram-positive and/or gram-negative bacteria, infection within 30 days of surgery/trauma with purulent drainage, onset of abscess within 7 days, onset of cellulitis in the prior 7 days, diabetic foot infections, or an infection associated with complications. Patients were randomized 2:1 to either IV ceftobiprole (500 mg infused over 120 minutes every 8 hours) plus placebo (n=547) or IV vancomycin (1,000 mg infused over 60 minutes every 12 hours) plus IV ceftazidime (1,000 mg infused over 120 minutes every 8 hours) (n=281). Therapy was continued for 7 to 14 days and clinical and microbiological evaluations were performed on Days 0, 4, 8, and 14. Of the 828 patients enrolled in the study, 590 were microbiologically evaluable. The most frequently identified isolated gram-positive cocci were MSSA, MRSA, pyogenes, and Staphylococcus epidermidis, and the most common gram-negative pathogens were E coli, P aeruginosa, E cloacae,P mirabilis, and K pneumoniae. Clinical cure was defined as the resolution of all signs and symptoms of the infection or improvement to such an extent that no further treatment was required for at least 5 days. The overall clinical cure rates demonstrated the noninferiority of ceftobiprole (83.6% for ceftobiprole vs 83% for vancomycin plus ceftazidime in the microbiological ITT population, and 90.8% vs 90.5% in the microbiologically evaluable population, respectively). In patients with concomitant bacteremia, 84.6% of patients treated with ceftobiprole achieved a clinical cure compared with 62.5% of patients treated with vancomycin plus ceftazidime. The clinical cure rates for patients with S aureus were similar between treatment groups. Ceftobiprole was associated with cure rates >75% against gram-negative bacteria. Moreover, the microbiological eradication rates were similar between patients treated with ceftobiprole and those treated with vancomycin plus ceftazidime (89% vs 91% for gram-positive pathogens and 85% vs 88% for gram-negative pathogens, respectively). Both of the treatment regimens were demonstrated to be safe and well tolerated, with similar rates of adverse events.
A subanalysis of the second phase 3 study focused on the enrolled patients with diabetic foot infections.28 In this population, the most commonly identified pathogens were MSSA, MRSA, E cloacae, Streptococcus agalactiae, P mirabilis, and P aeruginosa. The clinical cure rates in the clinically evaluable and ITT populations were comparable in both groups, but patients receiving ceftobiprole required a shorter duration of therapy compared with those receiving vancomycin plus ceftazidime (8.7 d vs 9.5 d; P<.05). Ceftobiprole was associated with higher rates of clinical cure compared with vancomycin plus ceftazidime (70.6% vs 53.8%) in patients with severe infections (defined according to the Infectious Diseases Society of America [IDSA] classification scheme).
Ceftobiprole's efficacy in treating pneumonia has been assessed in 2 phase 3 trials. Full study results have not yet been released; however, initial results are promising.29,30
ADVERSE EVENTS
Clinical studies have demonstrated that ceftobiprole is generally well tolerated with few adverse events. The most frequent drug-related adverse event was a transient caramel-like taste disturbance during infusion, which was probably caused by the conversion of the prodrug to the active antibiotic and the subsequent release of diacetyl, a substance known to have a caramel-buttery taste.5,7 The reported adverse events in one study were predominantly gastrointestinal (GI) events including nausea (14%), taste disturbance (8%), and vomiting (7%).26 Most of these adverse events were mild to moderate, and no significant differences in discontinuation rates were observed between treatment groups (ceftobiprole, 17 patients vs vancomycin, 22 patients).26
DRUG INTERACTIONS
Ceftobiprole has a low probability of causing significant drug-drug interactions because it does not induce or inhibit cytochrome P450 enzymes. Moreover, it is neither a substrate nor an inhibitor of P-glycoprotein.11 There are currently no published or presented clinical studies focusing on drug-drug interactions with ceftobiprole.
DOSING AND ADMINISTRATION
Although numerous doses of ceftobiprole have been evaluated, the proposed regimen for the treatment of cSSSIs is 500 mg every 8 hours, administered as a 2-hour infusion. In addition to the support of the phase 3 clinical trial data that demonstrated ceftobiprole's noninferiority to vancomycin, this dosage regimen has been supported by pharmacokinetic/pharmacodynamic models using Monte Carlo simulation, which aim to determine the probability that a ceftobiprole dosage regimen will attain a critical pharmacodynamic target based on actual dispersion from phase 1 and 2 studies and the MICs of the organism.9 In particular, for a dosing regimen of 500 mg every 12 hours infused over 60 minutes, the probabilities of achieving a nearly maximal bactericidal effect (defined as 50% fT>MIC in this analysis) for MSSA and MRSA were 96.9% and 92.6%, respectively. Increasing the dosage to 500 mg every 8 hours infused over 120 minutes resulted in a greater probability of achieving 50% fT>MIC for MRSA (98.8%) and MSSA (99.9%), and also provided a 94.1% probability of achieving 60% fT>MIC against non-AmpC-producing gram-negative bacilli, an 87.8% probability of achieving 60% fT>MIC against AmpC-producing gram-negative bacilli, and a 62% probability of achieving 60% fT>MIC against P aeruginosa isolates. Specifically, the probability of target attainment was observed to increase significantly at longer infusion durations when the ceftobiprole MIC was ≥2 mcg/mL. In patients with mild-to-moderate renal impairment (creatinine clearance ≤ 50 mL/min), the most appropriate treatment regimen was demonstrated to be 500 mg every 12 hours infused over 120 minutes.9 Further studies in patients with severe renal dysfunction are needed to establish dosing recommendations for these individuals, including those patients undergoing hemodialysis, peritoneal dialysis, or continuous renal replacement therapies.
Dr Kontou was a visiting scholar, Center for Anti-infective Research and Development, Hartford Hospital, Hartford, Connecticut, at the time this manuscript was prepared. She is now a pulmonologist at Papanikolaou Hospital, Thessaloniki, Greece. Dr Kuti is associate director, Clinical and Economic Studies, Center for Anti-infective Research and Development, Hartford Hospital. Dr Nicolau is director, Center for Anti-infective Research and Development, Hartford Hospital.
Disclosure Information: As related to products discussed in this article: Dr Kontou and Dr Kuti report no financial disclosures. Dr Nicolau has served on speakers' bureaus and as a consultant and periodically receives research support from AstraZeneca, Cubist, Merck, Johnson & Johnson, and Wyeth Pharmaceuticals.
In each issue, the "Focus on" feature reviews a newly approved or investigational drug of interest to pharmacy and therapeutics committee members. The column is coordinated by Robert A. Quercia, MS, RPh, clinical manager and director of Drug Information, Department of Pharmacy Services, Hartford Hospital, Hartford, Conn, and adjunct associate professor, University of Connecticut School of Pharmacy, Storrs, Conn; and by Craig I. Coleman, PharmD, assistant professor of pharmacy practice, University of Connecticut School of Pharmacy, and director, Pharmacoeconomics and Outcomes Studies Group, Hartford Hospital.
EDITORS' NOTE: The clinical information provided in "Focus on" articles is as current as possible. Due to regularly emerging data on developmental or newly approved drug therapies, articles include information published or presented and available to the author up until the time of the manuscript submission.
REFERENCES
1. Appelbaum PC. MRSA–the tip of the iceberg. Clin Microbiol Infect. 2006;12(suppl 2):3–10.
2. Deresinski S. Methicillin-resistant Staphylococcus aureus: An evolutionary, epidemiologic, and therapeutic odyssey. Clin Infect Dis. 2005;40: 562–573.
3. Moran GJ, Krishnadasan A, Gorwitz RJ, et al; for the EMERGEncy ID Net Study Group. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006;355:666–674.
4. Bush K, Heep M, Macielag MJ, Noel GJ. Anti-MRSA beta-lactams in development, with a focus on ceftobiprole: The first anti-MRSA beta-lactam to demonstrate clinical efficacy. Expert Opin Investig Drugs. 2007;16:419–429.
5. Schmitt-Hoffmann A, Roos B, Schleimer M, et al. Single-dose pharmacokinetics and safety of a novel broad-spectrum cephalosporin (BAL5788) in healthy volunteers. Antimicrob Agents Chemother. 2004;48:2570–2575.
6. Noel GJ. Clinical profile of ceftobiprole, a novel beta-lactam antibiotic. Clin Microbiol Infect. 2007;13(suppl 2):25–29.
7. Schmitt-Hoffmann A, Nyman L, Roos B, et al. Multiple-dose pharmacokinetics and safety of a novel broad-spectrum cephalosporin (BAL5788) in healthy volunteers. Antimicrob Agents Chemother. 2004;48:2576–2580.
8. Schmitt-Hoffmann AH, Roos B, Heep M, et al. Influence of gender on the pharmacokinetics of BAL9141 after intravenous infusion of pro-drug BAL5788. Presented at: 14th European Congress of Clinical Microbiology and Infectious Diseases; May 1–4, 2004; Prague, Czech Republic. Abstract P1030.
9. Lodise TP Jr, Pypstra R, Kahn JB, et al. Probability of target attainment for ceftobiprole as derived from a population pharmacokinetic analysis of 150 subjects. Antimicrob Agents Chemother. 2007;51:2378–2387.
10. Laohavaleeson S, Tessier PR, Nicolau DP. Pharmacodynamic characterization of ceftobiprole in pneumonia caused by phenotypically diverse Staphylococcus aureus. Presented at: 47th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; September 17–20, 2007; Chicago, IL. Abstract A-38.
11. Murthy B, Schmitt-Hoffmann A. Pharmacokinetics and pharmacodynamics of ceftobiprole, an anti-MRSA cephalosporin with broad-spectrum activity. Clin Pharmacokinet. 2008;47:21–33.
12. Lemaire S, Van Bambeke F, Glupczynski Y, Tulkens PM. Intraphagocytic activities of ceftobiprole vs conventional cephalosporins against methicillin-sensitive (MSSA) and methicillin-resistant S aureus (MRSA). Presented at: 47th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; September 17–20, 2007; Chicago, IL. Abstract A-1438.
13. Bogdanovich T, Ednie LM, Shapiro S, Appelbaum PC. Antistaphylococcal activity of ceftobiprole, a new broad-spectrum cephalosporin. Antimicrob Agents Chemother. 2005;49:4210–4219.
14. Kosowska K, Hoellman DB, Lin G, et al. Antipneumococcal activity of ceftobiprole, a novel broad-spectrum cephalosporin. Antimicrob Agents Chemother. 2005;49:1932–1942.
15. Arias CA, Singh KV, Panesso D, Murray BE. Time-kill and synergism studies of ceftobiprole against Enterococcus faecalis, including beta-lactamase-producing and vancomycin-resistant isolates. Antimicrob Agents Chemother. 2007;51:2043–2047.
16. Bogdanovich T, Clark C, Ednie L, et al. Activities of ceftobiprole, a novel broad-spectrum cephalosporin, against Haemophilus influenzae and Moraxella catarrhalis. Antimicrob Agents Chemother. 2106;50:2150–2157.
17. Hebeisen P, Heinze-Krauss I, Angehrn P, Hohl P, Page MG, Then RL. In vitro and in vivo properties of Ro 63-9141, a novel broad-spectrum cephalosporin with activity against methicillin-resistant staphylococci. Antimicrob Agents Chemother. 2001;45:825–836.
18. Leonard SN, Cheung CM, Rybak MJ. In vitro activity of ceftobiprole (CEF) against clinical isolates of hospital (HA) and community-acquired (CA) methicillin-resistant Staphylococcus aureus (MRSA). Presented at: 47th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; September 17–20, 2007; Chicago, IL. Abstract E-278.
19. Denis O, Deplano A, Nonhoff C, et al. In vitro activities of ceftobiprole, tigecycline, daptomycin, and 19 other antimicrobials against methicillin-resistant Staphylococcus aureus strains from a national survey of Belgian hospitals. Antimicrob Agents Chemother. 2006;50:2680–2685.
20. Deshpande LM, Jones RN. Bactericidal activity and synergy studies of BAL9141, a novel pyrrolidinone-3-ylidenemethyl cephem, tested against streptococci, enterococci and methicillin-resistant staphylococci. Clin Microbiol Infect. 2003;9:1120–1124.
21. Queenan AM, Shang W, Kania M, Page MGP, Bush K. Interactions of ceftobiprole with beta-lactamases from molecular classes A to D. Antimicrob Agents Chemother. 2007;51:3089–3095.
22. Brown NP, Jones ME, Draghi DC, Cohen MA, Thornsberry C, Sahm DF. Baseline surveillance profiles of ceftobiprole (BPR) activity against Enterobacteriaceae and P aeruginosa (PA). Poster presented at: 46th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; September 27–30, 2006; San Francisco, CA. Poster E-112.
23. Fritsche TR, Sader HS, Jones RN. In vitro activity of ceftobiprole tested against a recent collection of North American Pseudomonas aeruginosa. Poster presented at: 46th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; September 27–30, 2006; San Francisco, CA. Poster E-115.
24. Goldstein EJC, Citron DM, Merriam CV, Warren YA, Tyrrell KL, Fernandez HT. In vitro activity of ceftobiprole against aerobic and anaerobic strains isolated from diabetic foot infections. Antimicrob Agents Chemother. 2006;50:3959–3962.
25. Heep M, Querner S, Harsch M, O'Riordan W. BAL5788, the first of a new class of anti-MRSA cephalosporins: Microbiological results from a phase II study in complicated skin and skin structure infections. Presented at: 44th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; October 30–November 2, 2004; Washington, DC. Abstract L-361.
26. Noel GJ, Strauss RS, Amsler K, Heep M, Pypstra R, Solomkin JS. Results of a double-blind, randomized trial of ceftobiprole treatment of complicated skin and skin structure infections caused by gram-positive bacteria. Antimicrob Agents Chemother. 2008;52:37–44.
27. Strauss RS, Bagchi P, Noel GJ. Ceftobiprole (BPR) as treatment of complicated skin structure infections (cSSSI) caused by gram-negative infections, including Pseudomonas aeruginosa (PsA). Presented at: 45th Annual Meeting of the Infectious Diseases Society of America; October 4–7, 2007; San Diego, CA. Abstract 1094.
28. Strauss RS, Bagchi P, Noel GJ. Ceftobiprole (BPR) compared to vancomycin plus ceftazidime (VAN+CAZ) in treatment of diabetic patients with mild, moderate and severe foot infections. Presented at: 45th Annual Meeting of the Infectious Diseases Society of America; October 4–7, 2007; San Diego, CA. Abstract 1086.
29. Basilea announces positive top-line data from phase III study of ceftobiprole in community-acquired pneumonia requiring hospitalization [press release]. Basel, Switzerland: Basilea Pharmaceutica, Ltd; September 14, 2007. http://www.basilea.com/template_loader.php?tplpage_id=34&mode=details&id=131. Accessed January 17, 2008.
30. Basilea announces positive top-line data from phase III study of ceftobiprole in hospital-acquired pneumonia [press release]. Basel, Switzerland: Basilea Pharmaceutica, Ltd; October 9, 2007. http://www.basilea.com/template_loader.php?tplpage_id=34&mode=details&id=144. Accessed January 17, 2008.

Employers Face Barriers With Adopting Biosimilars
March 1st 2022Despite the promise of savings billions of dollars in the United States, adoption of biosimilars has been slow. A roundtable discussion among employers highlighted some of the barriers, including formulary design and drug pricing and rebates.






