
- Safety & Recalls
- Regulatory Updates
- Drug Coverage
- COPD
- Cardiovascular
- Obstetrics-Gynecology & Women's Health
- Ophthalmology
- Clinical Pharmacology
- Pediatrics
- Urology
- Pharmacy
- Idiopathic Pulmonary Fibrosis
- Diabetes and Endocrinology
- Allergy, Immunology, and ENT
- Musculoskeletal/Rheumatology
- Respiratory
- Psychiatry and Behavioral Health
- Dermatology
- Oncology
Etravirine: A unique non-nucleoside reverse transcriptase inhibitor for the treatment of HIV-1
Etravirine is an HIV-1 specific, non-nucleoside reverse transcriptase inhibitor (NNRTI) that was FDA approved for treatment-experienced adult patients with HIV-1 strains resistant to an NNRTI and other antiretroviral agents. In phase 3 trials of etravirine versus placebo, both in combination with darunavir/ritonavir, a background of nucleoside/nucleotide reverse transcriptase inhibitors with or without enfuvirtide demonstrated potent antiviral activity that was sustained through 48 weeks.



Key Points
Abstract
Etravirine is an HIV-1 specific, non-nucleoside reverse transcriptase inhibitor (NNRTI) that was FDA approved for treatment-experienced adult patients with HIV-1 strains resistant to an NNRTI and other antiretroviral agents. In phase 3 trials of etravirine versus placebo, both in combination with darunavir/ritonavir, a background of nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs) with or without enfuvirtide demonstrated potent antiviral activity that was sustained through 48 weeks. Specifically, the patients in the etravirine group were more likely to achieve the primary outcome of a viral load <50 copies/mL at 24 weeks, which was sustained through 48 weeks. The most common adverse effects reported in phase 3 studies were rash, diarrhea, nausea, nasopharyngitis, headache, and injection site reaction. Although many patients continued therapy despite the rash, 2.2% of total patients in the phase 3 studies discontinued the trial due to the rash. Additionally, post-marketing reports have described cases of toxic epidermal necrolysis and hypersensitivity reactions. Like many antiretroviral agents, etravirine has a variety of drug interactions. It is a known substrate of CYP3A, 2D6, and 2C19 as well as an inducer of CYP3A, 2C9, 2C19, and P-glycoprotein. Because of the drug interactions, etravirine should not be given in combination with any NNRTI, a protease inhibitor without ritonavir, or with tipranavir/ritonavir, fosamprenavir/ritonavir, atazanavir/ritonavir, or ritonavir (except as a boosting agent). (Formulary. 2010;45:78–83; 101–103.)
Currently about 33 million persons are infected with HIV worldwide, with about 2.7 million persons acquiring the disease in 2007.1 Although there has been a slight decrease in the number of cases and deaths due to HIV and AIDS worldwide since the last report in the early 2000s, it is important to continue to seek newer antiretroviral agents to provide patients with additional options, especially against resistant viruses.
Etravirine is an HIV-1 specific NNRTI that was approved by FDA on January 18, 2008. It was approved as part of combination therapy for HIV-1 infection in treatment-experienced adults who have evidence of viral replication and HIV-1 strains resistant to an NNRTI and other antiretroviral agents.3,4
CHEMISTRY AND PHARMACOLOGY
Etravirine (4-[[6-amino-5-bromo-2-[(4-cyanophenyl)amino]-4-pyrimidinyl]oxy]-3,5-dimethylbenzonitrile) has a molecular formula of C20H15BrN6O and a molecular weight of 435.28 g/mol.3,4
Etravirine is very lipid soluble and as such produces issues with bioavailability. Etravirine must be taken with food to increase the solubility and gastric residence time.5 The first formulation of etravirine used in phase 2 trials was a granulolayered formulation that was associated with increased patient variability and high pill burden.6 To improve these factors a spray-dried technique was used beginning in phase 3 trials and is now the formulation that is marketed. This formulation is available as 100-mg tablets and is recommended to be given 200 mg twice a day.3
Clinically, the unique qualities of etravirine are due to its flexibility in binding, which results in activity against many viruses that are resistant to the rest of the NNRTI class.7
RESISTANCE ANALYSIS
As of December 2009, there are 17 mutations associated with etravirine (V90I, A98G, L100I, K101E/H/P, V106I, E138A, V179D/F/T, Y181C/I/V, G190A/S, and M230L) based on the International AIDS Society-USA drug resistance mutation list.8 The prevalence of each mutation has been evaluated in multiple studies. It appears that etravirine resistance is more associated with the number and types of resistance mutations. As such prediction estimates related to clinical response and susceptibility to etravirine have been developed. The most comprehensive evaluation has determined both a clinical cut-off (CCO) for etravirine fold change effective concentration (EC50) and a weighted genotypic score based on the fold change and clinical response data.9 The analysis evaluated pooled data at week 24 from 403 patients who received etravirine (but were not receiving enfuvirtide de novo) in the TMC125 to Demonstrate Undetectable viral load in patients Experienced with ARV Therapy (DUET)-1 and DUET-2 phase 3 clinical trials. Both a lower and a preliminary upper baseline CCO were determined for etravirine based on virologic response rates (HIV viral load <50 copies/mL) when used as a part of darunavir- or ritonavir-based therapy (DUET study design). Many patients did not have EC50 fold changes >13, so a formal upper baseline CCO could not be established.9
A weighted genotypic scoring system was created using the pooled DUET study data and data from 4,248 clinical isolates with NNRTI-resistant isolates.9 The score system provides a score from 1 to 4 to each of the 17 resistance mutations. All of the points are summed to create a total score. Total scores of ≤2.0 have the highest likelihood of response (74%), scores of 2.5 through 3.5 have an intermediate response (52%), and scores >4.0 have reduced response (38%).9 Alternative weighting methods to determine reduced response have also been reported. These alternative methods were created using DUET data or another large clinical data set and developed as genotypic interpretation systems.12,13 These alternative methods showed good concordance with the pooled analysis weighting system described earlier.9,14
Although not established as an etravirine mutation, one report suggests that N348I (especially in the presence of Y181C) as well as E138A/G/Q may also potentially decrease etravirine response rate.15,16 Another report suggests that similar to other NNRTIs, nucleoside-associated mutations and/or the M184V mutation may be associated with a hypersensitivity to etravirine.17
One study investigated the likelihood of cross-resistance between etravirine and either of the first-generation NNRTIs, nevirapine or efavirenz. Their evaluation suggests that prior therapy with nevirapine was associated with an increased rate of resistance mutations compared to efavirenz.18
PHARMACOKINETICS

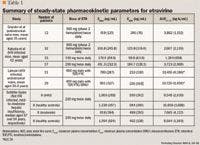
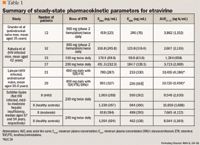
Etravirine should be taken with food to enhance bioavailability; the standard breakfast reported is 4 slices of bread, 2 slices of ham or cheese, butter, jelly, and 2 cups of decaffeinated coffee or tea with milk and/or sugar.5,6 A recent study evaluated the effects of various meals on the single-dose pharmacokinetics of etravirine.5 The study demonstrated significant decreases in both maximum plasma concentration (Cmax) and area under the curve (AUC) for subjects who took etravirine in a fasted state (decrease Cmax 44% and AUC 51%) or after receiving a high-fiber breakfast containing fruits, 2 slices of bread, jam, and orange juice (decrease Cmax 38% and AUC 25%), while the light breakfast (croissant, butter, jam, and a cup tea or coffee) demonstrated significant reductions in AUC only (20% decrease).5 Subjects in the high-fat group (eggs, bacon, croissant, bread, butter, chocolate, and cup of tea or coffee) had similar exposures to the standard breakfast controls. The decrease in AUC for the light breakfast is worth noting as this breakfast had higher fat than the standard breakfast (17.4 g vs 15.3 g), but was lower in protein (5.2 g vs 21.9 g).5
PEDIATRICS
To evaluate the pharmacokinetics of etravirine in children, alternative dosage forms reviewed included a pediatric tablet that was 25 mg and compositionally proportional to the adult 100-mg tablet, as well as crushing and dissolving in water of the adult 100-mg tablet.22 Specifically the bioavailability in healthy adults was determined for 100 mg of each formulation and compared with the currently marketed formulation. The AUC of both formulations was considered similar. Although the Cmax for the 4 pediatric tablets was slightly lower than the traditional formulation, it was not believed to result in any difference.
Etravirine pharmacokinetics using a dose of 4 mg/kg twice daily have been evaluated in 16 children between 6 and 17 years of age.23 Cmax was 555 ng/mL (SD 515 ng/mL), minimum plasma concentration (Cmin) was 233 ng/mL (SD 238 ng/mL), and AUC12h 4,788 (SD 4,459 ng·h/mL). Although statistically the concentrations were similar to adult concentrations, increased interpatient variability not clearly related to age or body surface area was seen and concern remains about underdosing pediatric HIV patients. As a result, a higher dose of 5.2 mg/kg twice daily is now being evaluated in phase 2 trials.23
Only a single case report is available describing the use of etravirine in a patient younger than 6 years. A 2-year-old child was begun on etravirine at a dose of 50 mg twice daily. At day 7 his pre-dose concentration was determined to be 26.3 ng/mL, which led to an increased dose of 100 mg twice daily with a repeat pre-dose level of 650 ng/mL.24
PREGNANCY
Currently data regarding the pharmacokinetics of etravirine during pregnancy are being investigated. One case report describes the use of the adult dose in a pregnant 38-year-old woman with multidrug-resistant HIV.25 Her steady-state peak was 1,201 ng/mL and Cmin was 896 ng/mL. Additionally the etravirine had detectible levels (345 ng/mL and 414 ng/mL) in the cord blood of her twin babies.25 In another small study the pharmacokinetics and outcomes of etravirine in the third trimester were presented for 5 babies.26 The pharmacokinetics in the pregnant women were found to be comparable to the pharmacokinetics in non-pregnant adults.
ORGAN DYSFUNCTION
The pharmacokinetics of etravirine have not been studied in patients with severe hepatic dysfunction or in those receiving hemodialysis. A case report describing a 49-year-old HIV patient requiring hemodialysis had therapeutic drug monitoring of his HIV therapy, including etravirine. His etravirine level prior to hemodialysis was 380 ng/mL and 270 ng/mL post dialysis (just prior to his morning dose). This case suggests that for this patient the hemodialysis results in <30% reduction in etravirine concentrations.27
Evaluations in patients with mild-to-moderate hepatic dysfunction do not suggest modifying the dose of etravirine.19 Potential concern, however, exists regarding the use of etravirine in patients with severe liver dysfunction due to a lack of data, as well as a case report describing extremely high etravirine concentrations (3,257 ng/mL) and prolonged half-life (237 h) in a patient with decompensated liver disease.28
CLINICAL TRIALS



Phase 2 studies. The first phase 2 study of etravirine included generally healthy antiretroviral naïve HIV-positive men with an HIV viral load of 5,000 to 125,000.21 Subjects were stratified in a 2:1 ratio to receive either twice-daily etravirine (phase 2 formulation) at a dose of 900 mg or matched placebo as monotherapy for 7 days. The primary objective was change of viral load from baseline, which was significantly lower in the subjects who received etravirine compared with those who received placebo. Additionally, subjects who received etravirine versus placebo were also more likely to have 1 log10 decrease or greater in HIV viral load, increased CD4 cell counts, and a viral load of <400 copies/mL.
The second phase 2 study was an international study that compared etravirine at 400 mg, 800 mg, or 1,200 mg (dose escalation study) twice daily plus an investigator-chosen antiretroviral background compared to just an investigator-chosen antiretroviral background regimen.29 Adult subjects were eligible if they were HIV positive with a viral load of 1,000 copies/mL or greater, generally healthy, had no history of an allergic reaction to NNRTI or abacavir, and had previously received (≥3 months) NNRTIs, NRTIs, and PIs. Additionally, their antiretroviral therapy had to be stable for the past 8 weeks. The aims of the study were to determine etravirine's antiretroviral activity and safety and tolerability.
The study was conducted in 2 stages to phase in the dose. In the first stage, patients were randomly assigned 1:1:1 to placebo or etravirine 400 mg twice daily or 800 mg twice daily for 48 weeks, whereas in stage 2 patients were randomly assigned in a 1:2:4 ratio to placebo or etravirine 800 mg twice daily or 1,200 mg twice daily for 48 weeks. Patients were allowed to continue the regimen for an additional 96 weeks. A total of 240 patients (166 stage 1 and 74 stage 2; placebo n=66, 400 mg n=57, 800 mg n=43, 1,200 mg n=43) were randomly assigned and included in the intent-to-treat analysis. In stage 1, no differences were observed for change in log10 viral load at 24 weeks or CD4 cell counts at 48 weeks in any group. Investigators suggest that stage 1 results may have been influenced by a lab technique that was fixed for stage 2 as well as a lack of standardization defining background regimen. The study had a significant amendment between stage 1 and stage 2 that improved the lab technique as well as modified the definition of optimized background regimen to make all control and etravirine groups more similar. In stage 2, both the 800-mg (P=.009) and the 1,200-mg (P=.049) groups demonstrated improvements in clinical markers including decreases in log10 viral load at 24 weeks (trend at 48 weeks) and increases in CD4 cell count at 48 weeks compared with placebo (800 mg, P=.25; 1,200 mg, P=.019).29
Another phase 2 study conducted from April to November 2004 randomly assigned patients 2:2:1 to receive etravirine 400 mg twice daily, 800 mg twice daily, or placebo for 24 weeks with an optimized antiretroviral background regimen.30 For the etravirine group the optimized background included at least 2 of the following: NRTI, lopinavir/ritonavir, or enfuvirtide. The control group required at least 3 of the following: NRTIs, PIs, and enfuvirtide. Patients were included if they had multidrug-resistant HIV virus (≥1 NNRTI mutation, ≥3 primary PI mutations, ≥3 months NRTI experience) and HIV viral load of 1,000 copies/mL or greater. Those with evidence of significant hepatic or renal compromise, cutaneous reaction to a prior NNRTI, or any grade 3 or 4 lab abnormalities were excluded.
In an intent-to-treat analysis 199 patients were enrolled. The mean viral load change from baseline was significantly greater for both 400 mg (P =.005) and 800 mg (P<.001) compared with placebo. Additionally, the percentage of patients with a viral load decrease of 1.0 log10 or more and the number of patients with a viral load <400 copies/mL were also statistically more likely for patients in both active groups compared with placebo (no difference was seen between active groups). Finally, no differences were seen between groups for percent of patients who achieved viral loads <50 copies/mL.30
Etravirine was evaluated between March 2005 and July 2006 in an international study to determine its effectiveness in NNRTI-resistant, PI-naïve patients.31 Patients from South Africa, Thailand, Brazil, and Mexico were randomly assigned equally to receive either etravirine 800 mg twice daily with food or an investigator-chosen PI. Both groups also received 2 investigator-chosen NRTIs. Since the efficacy in this population was uncertain, clinical outcomes such as viral load and CD4 counts and safety assessments were monitored at baseline (2 weeks for viral load) and 4 weeks, and every 4 weeks thereafter for 24 weeks. The study included 116 patients. The trial was stopped early and patients in the etravirine group were switched because of an interim analysis showing that etravirine response was worse than that seen in the control group. The investigators hypothesize that the response may have been because of baseline resistance in the etravirine group.31
Final phase 2 study. The final phase 2 study occurred between May and August 2007 and was a noncomparative single-dose study investigating the use of etravirine 200 mg twice daily (newer formulation) with raltegravir 400 mg twice daily and darunavir/ritonavir 600 mg/100 mg twice daily with or without additional NRTIs and/or enfuvirtide.32 The study included patients with viral loads 1,000 copies/mL or more, at least 3 PI mutations, and 3 NRTI resistance mutations or more, but who were susceptible to darunavir and etravirine. The patients also could not have received any of the 3 included agents in the study and were on a stable regimen for at least 8 weeks before study entry. Exclusion criteria were stricter than prior studies excluding all patients with current AIDS-defining illness or cancer, or who were pregnant, breastfeeding, or of childbearing age. Additionally, the study had strict lab criteria that did not allow for neutropenia, thrombocytopenia, hemoglobin less than 7 mg/dL, severe (<50 mL/min) active liver dysfunction (hepatitis B or C were allowed if they had normal to mild hepatic insufficiency), and <3 times elevations of liver function tests.
A total of 103 patients were enrolled in the study. As part of their regimen, 84% of patients received NRTIs and 12% received enfuvirtide. The primary outcome was an HIV viral load <50 copies/mL at 24 weeks, which 90% of subjects achieved. Secondary outcomes measures of HIV viral load <50 copies/mL at 48 weeks, change in HIV viral load, and CD4 counts from baseline to week 48 were also reported (Table 2). Two new AIDS-defining events were noted-HIV encephalopathy and esophageal candidiasis.32
Phase 3 studies. The two major phase 3 studies associated with etravirine's FDA approval were DUET-1 and DUET-2.33-35 These studies, conducted between November 2005 and July 2006, vary only based on the locations of patients. DUET-1 enrolled patients in Argentina, Brazil, Chile, France, Mexico, Panama, Puerto Rico, Thailand, and the United States, whereas DUET-2 recruited patients in Australia, Belgium, Canada, France, Germany, Italy, Netherlands, Poland, Portugal, Spain, United Kingdom, and the United States.33-35 Both studies evaluated adult HIV patients on stable antiretroviral therapy with viral loads >5,000 copies/mL who had multidrug-resistant virus (≥1 NNRTI mutation and ≥3 primary PI mutations). Patients in the studies were randomized to receive either etravirine or placebo. In DUET-1, 612 patients received treatment, while in DUET-2, 591 patients received treatment. All patients received at least 2 NRTIs as determined by the investigators and darunavir/ritonavir 600 mg/100 mg twice daily. Enfuvirtide was optional for all patients. The primary outcome was the percentage of patients who achieved an HIV viral load <50 copies/mL at week 24. Secondary end points included change in viral load from baseline, percentage of patients with viral load <400 copies/mL, and changes in CD4 cell counts. The study specifics are shown in Table 2. Those receiving etravirine in both DUET-1 and DUET-2 were more likely to reach the primary goal of viral load <50 copies/mL (DUET-1: 56% etravirine vs 39% placebo, P=.005; DUET-2: 62% etravirine vs 44% placebo, P=.003). Additionally, both studies demonstrated higher mean change in viral load from baseline and higher average change in CD4 cell counts for the etravirine groups.33-35
A subanalysis was conducted to evaluate the effect of enfuvirtide use on outcomes. Of the patients for whom enfuvirtide was new, the DUET-1 study did not demonstrate a difference at 24 weeks between the etravirine and placebo groups for HIV viral loads <50 or 400 copies/mL. The DUET-2 study as well as the 48-week combined data had conflicting results demonstrating more patients in the etravirine group achieving viral loads <400 copies/mL (combined 48-week analysis only) and 50 copies/mL (both DUET-2, and combined 48-week DUET-1 and DUET-2).33-35
In addition to the DUET studies early access phase 3 study results have been reported. TMC125-C214 studies were designed for patients who had failed multiple regimens with limited treatment options.36,37 Study objectives were to observe safety and tolerability as well as efficacy when etravirine was combined with other antiretroviral agents. These other antiretroviral agents were determined by the investigator, but could include: boosted darunavir, lopinavir, atazanavir, fosamprenavir, indinavir, saquinavir, approved NRTIs, and enfuvirtide. Maraviroc and raltegravir were permitted 1 year into the early access program. The first study describes the 48-week data for 2,578 patients who received etravirine in the United States early access program.36 Patients were evaluated based on other strong new antiretroviral use: 38% etravirine plus darunavir/ritonavir and raltegravir, 24% etravirine plus just darunavir/ritonavir, 19% etravirine plus raltegravir, and 19% etravirine without either darunavir/ritonavir or raltegravir. Almost 80% of patients had a <1 log10 copies/mL reduction in viral load, 62% achieving viral loads <75 copies/mL, and had a median increase in CD4 cell count of about 100 cells/mm3. The second study reported the 24-week data from 22 patients in Europe and 15 patients in Canada.37 All of these patients had viral loads <50 copies/mL at baseline. In addition to etravirine, most patients also received darunavir (n=36) and raltegravir (n=23). For about half of the patients the major switch was from enfuvirtide to etravirine. Overall, the analysis showed most patients continued to do well, with 95% having viral loads <50 copies/mL at 24 weeks and mean increase in CD4 count of 26 cells/mm3. It should be noted that the 2 patients who did not have viral loads <50 copies/mL at week 24 included 1 whose viral load was 50 copies/mL and 1 patient lost to follow-up who had achieved this goal previously. Subgroup patients switched from enfuvirtide to etravirine also appeared to do well.
The last early access study was from Spain, and it evaluated etravirine as part of HIV salvage therapy with raltegravir and darunavir/ritonavir in 32 HIV-1 patients for 24 weeks.38 Of the intent-to-treat population, 94% achieved viral loads <50 copies/mL. Additionally, CD4 cell counts increased by a median of 103 cells/mm3.
SAFETY AND TOLERABILITY
In phase 3 clinical trials 1,203 patients received etravirine (DUET-1 and DUET-2).33-35 An additional 2,578 patients in the United States, 22 in Europe, and 15 in Canada received etravirine as part of early access.36,37 In these studies the most common adverse effects occurring in 10% to 20% of etravirine-treated patients (regardless of association) were: rash, diarrhea, nausea, nasopharyngitis, headache, and injection-site reaction.35 Diarrhea, nausea, and rash occurred at grade 2 or greater in 5% to 10% of patients. No differences between groups were seen for neuropsychiatric events or laboratory abnormalities including liver function tests, pancreatic enzymes, or cholesterol.35 Similar findings were seen in the early access evaluations, with rash being the most common adverse event. Additionally, these early access programs had 2 cases of Stevens-Johnson syndrome that occurred in patients receiving the medication. Eight patients (0.3%) in the early access program died of an adverse event defined as at least possibly related to the etravirine. These adverse effects resulting in death were reported as: pancreatitis, pancytopenia, AIDS, hepatitis B, vomiting, multiple organ failure, hepatic cirrhosis, and hepatic failure.
About 19% of patients receiving etravirine had a rash in the DUET-1 and DUET-2 studies.33-35 The rash usually was maculopapular or erythematous, occurred commonly in week 2 of treatment, and resolved after 1 or 2 weeks of continued therapy. The discontinuation rate due to rash was 2.2%. In the DUET studies no cases of Stevens-Johnson syndrome were seen in the etravirine group, but 1 occurred in the placebo group. The early access studies also reported 2 cases of Stevens-Johnson syndrome. Additionally, post-marketing surveillance reported cases of toxic epidermal necrolysis and hypersensitivity reactions that sometimes also included hepatic failure.3
Researchers also evaluated the effect of etravirine on the QTc.39 Etravirine was administered as either 200 mg twice daily or 400 mg once daily to healthy volunteers in separate 8-day sessions, followed by a 14-day or longer washout period. Controls were moxifloxacin 400 mg once daily and placebo. The study reported that neither dose of etravirine prolonged the QTc.
Special populations. In rat studies, proportional to clinical doses, etravirine did not appear to have any effect on embryo-fetal development.40
Additionally, 6 human babies from 5 pregnancies in which the mother received etravirine were found to be healthy, with the only malformation an accessory auricle.26 Currently etravirine is classified as a pregnancy category B drug and has an antiretroviral pregnancy registry to continue to obtain data from women who receive it when pregnant (1-800-258-4263).3
In the pediatric pharmacokinetics trial, no patients discontinued therapy due to an adverse event.23 Similar to the adult data, rash was the most common adverse event, occurring in 2 of 16 patients. No other adverse effects or laboratory abnormalities were noted.23
DRUG INTERACTIONS
Like many HIV antiretroviral drugs, etravirine has numerous drug interactions. Specifically, etravirine is known to be a substrate of CYP3A, 2D6, and 2C19 as well as an inducer of CYP3A, 2C9, 2C19, and P-glycoprotein.3 Additionally, due to expected interactions, caution and close monitoring (including drug level monitoring when appropriate) should be used when administering etravirine with other drugs that are known to be inducers, inhibitors, or substrates of these pathways.

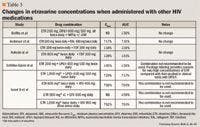
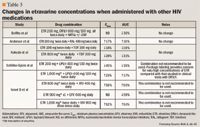
Etravirine has also been well studied with other medications to assess interactions including: ethinyl estradiol/norethindrone, digoxin, methadone, omeprazole, and ranitidine. No interaction was demonstrated for the ethinyl estradiol/norethindrone, omeprazole, or ranitidine.47,48 The only noted significant difference demonstrated between methadone (60–120 mg daily) and etravirine (100 mg twice daily) after 2 weeks of concurrent administration was the C0h value for the S-methadone isomer as compared to baseline.49 The authors did not consider this clinically relevant as the isomer is inactive and none of the patients experienced any signs of withdrawal. The product labeling does suggest, however, that patients need to be monitored clinically for any potential signs of withdrawal.3
Digoxin was also evaluated to determine the effect of the drug combination. Healthy volunteers were given digoxin (0.5 mg daily) and etravirine (200 mg twice daily), with increases of 19% and 18% observed for Cmax and AUClast, respectively.50 Although no dose adjustments are recommended, patients should be initiated on the lowest dose of digoxin and therapeutic monitoring of digoxin should be undertaken in both new and continuing patients.
DOSAGE AND ADMINISTRATION
Etravirine is FDA approved to be used in combination with other HIV-1 therapies in treatment-experienced adults with evidence of viral replication and HIV-1 strains resistant to an NNRTI and other antiretroviral agents.3 In these patients the dose is two 100-mg tablets taken twice daily after a meal.
Special populations. No dose adjustments are suggested for renal dysfunction or mild-to-moderate hepatic dysfunction. Limited data are available in pregnancy; currently no dose adjustment is suggested for pregnant women. The dosing for pediatric patients has not been established, but is being investigated at a dose of 5.2 mg/kg twice daily.
FORMULARY CONSIDERATIONS
Many agents are currently approved by the FDA for treatment of HIV. Etravirine, like many of the currently approved medications, is approved for patients who are treatment experienced. Therapies such as etravirine are needed for treatment-experienced patients who often have HIV that is resistant to many if not most other therapies or are intolerant to individual or classes of antiretroviral agents.
Etravirine is unique among the NNRTIs because it requires different mutations to confer resistance. In the past if a patient was resistant to a single NNRTI it would eliminate the entire class.
Etravirine, although studied in different populations, appears to have the most beneficial effect when combined with other potent agents (such as darunavir/ritonavir and NRTIs with or without enfuvirtide in the DUET studies) in treatment-experienced patients with HIV resistant to many drugs or classes. When combined in this manner in the DUET trials, it was able to demonstrate the primary and secondary outcomes of a sustained viral load <50 copies/mL for 24 and 48 weeks versus placebo.
Overall etravirine is well tolerated. The most common adverse effects reported in phase 3 trials occurred in 10% to 20% of patients and included rash, diarrhea, nausea, nasopharyngitis, headache, and injection site reaction. The most common reason for study discontinuation was rash, which occurred in 2.2% of the subjects. Additionally although not common, post-marketing surveillance has revealed that severe skin and hypersensitivity reactions are possible with etravirine.
Etravirine is dosed at 200 mg (two 100-mg tablets) twice daily with food. Pharmacokinetic data suggest that the tablets can be crushed and put into water (rinsing and drinking the remaining to ensure the whole dose is given). The average wholesale price of etravirine is about $30 per day, which is less than most new agents.
There are many known drug interactions. Etravirine is both a substrate of CYP3A, 2D6, and 2C19, and an inducer of CYP3A, 2C9, 2C19, and P-glycoprotein. It should not be co-administered with any NNRTI, a PI without ritonavir, or with tipranavir/ritonavir, fosamprenavir/ritonavir, atazanavir/ritonavir, or ritonavir (except as a boosting agent).
Etravirine's role in the treatment of HIV-1 is in the treatment-experienced population against multiple drug-resistant HIV (including virus resistant to the other NNRTIs). Etravirine is most useful when it is part of a new regimen that consists of at least 1 other active agent (such as darunavir/ritonavir in the DUET studies).
Dr Girotto is assistant clinical professor, University of Connecticut School of Pharmacy, Storrs, Conn., and clinical pharmacy specialist, department of pharmacy and division of pediatric infectious diseases, Connecticut Children's Medical Center, Hartford, Conn.
Disclosure Information: The author reports no financial disclosures as related to products discussed in this article.
In each issue, the "Focus on" feature reviews a newly approved or investigational drug of interest to pharmacy and therapeutics committee members. The column is coordinated by Robert A. Quercia, MS, RPh, clinical manager, Department of Pharmacy Services, Hartford Hospital, Hartford, Conn, and adjunct associate professor, University of Connecticut School of Pharmacy, Storrs, Conn; and by Craig I. Coleman, PharmD, associate professor of pharmacy practice, University of Connecticut School of Pharmacy, and director, Pharmacoeconomics and Outcomes Studies Group, Hartford Hospital.
EDITORS' NOTE: The clinical information provided in "Focus on" articles is as current as possible. Due to regularly emerging data on developmental or newly approved drug therapies, articles include information published or presented and available to the author up until the time of the manuscript submission.
REFERENCES
1. World Health Organization. Executive summary: 2008 Report on the global AIDS epidemic. Available at: http://www.unaids.org/en/KnowledgeCentre/HIVData/GlobalReport/2008/2008_Global_report.asp. Accessed February 23, 2010.
2. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. December 1, 2009; 1–161. Available at http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed February 23, 2010.
3. Intelence [package insert]. Raritan, NJ: Tibotec Therapeutics; November 2009.
4. ChemIDPlus. Available at: http://chem.sis.nlm.nih.gov/chemidplus/chemidlite.jsp. Accessed February 23, 2010.
5. Schöller-Gyüre M, Boffito M, Pozniak AL, et al. Effects of different meal compositions and fasted state on the oral bioavailability of etravirine. Pharmacotherapy. 2008;28:1215–1222.
6. Kakuda TN, Schöller-Gyüre M, Workman C, et al. Single- and multiple-dose pharmacokinetics of etravirine administered as two different formulations in HIV-1 infected patients. Antivir Ther. 2008;13:655–661.
7. Das K, Clark AD Jr, Lewi PJ, et al. Roles of conformational and positional adaptability in structure-based design of TMC125-R165335 (etravirine) and related non-nucleoside reverse transcriptase inhibitors that are highly potent and effective against wild-type and drug-resistant HIV-1 variants. J Med Chem. 2004;47:2550–2560.
8. Johnson VA, Brun-Vézinet F, Clotet B, et al. Update of the drug resistance mutations in HIV-1: December 2009. Top HIV Med. 2009;17:138–145.
9. Vingerhoets J, Tambuyzer L, Azijn H, et al. Resistance profile of etravirine: combined analysis of baseline genotypic and phenotypic data from the randomized, controlled phase III clinical studies. AIDS. 2010;24:503–514.
10. Poveda E, Garrido C, de Mendoza C, et al. Prevalence of etravirine (TMC-125) resistance mutations in HIV-infected patients with prior experience of non-nucleoside reverse transcriptase inhibitors. J Antimicrob Chemother. 2007;60:1409–1410.
11. Llibre JM, Santos JR, Puig T, et al. Prevalence of etravirine-associated mutations in clinical samples with resistance to nevirapine and efavirenz. J Antimicrob Chemother. 2008;62:909–913.
12. Bacheler L, Van Der Borght K, Van Craenenbroeck E, Winters B, Lecocq P. Exploring etravirine resistance among recent routine clinical samples submitted for resistance testing. Antivir Ther. 2008;13(suppl 3):A120.
13. Benhamida J, Chappey C, Coakley E, Parkin NT. HIV-1 genotype algorithms for prediction of etravirine susceptibility: novel mutations and weighting factors identified through correlations to phenotype. Antivir Ther. 2008;13(suppl 3):A142.
14. Tambuyzer L, Vingerhoets J, Azijn H, et al. Comparison of two ETR weighted genotypic scores with phenotypic susceptibility and virologic response data. 7th European HIV Drug Resistance Workshop, Stockholm, Sweden, March 25-27, 2009. Abstract 114.
15. Sluis-Cremer N, Moore K, Radzio J, Sonza S, Tachedjian G. N348I in HIV-1 reverse transcriptase decreases susceptibility to tenofovir and etravirine in combination with other resistance mutations. AIDS. 2010;24:317–319.
16. Kagan RM, Sista P, Pattery T, Bacheler L, Schwab DA. Additional HIV-1 mutation patterns associated with reduced phenotypic susceptibility to etravirine in clinical samples. AIDS. 2009;23:1602–1605.
17. Picchio G, Vingerhoets J, Parkin NT, Azijn H, de Bethune MP. Nucleoside-associated mutations cause hypersusceptibility to etravirine. Antivir Ther. 2008;13(suppl 3):A25.
18. Manosuthi W, Butler DM, Chantratita W, et al. Mutations associated with etravirine resistance among patients infected with HIV-1 subtype CRF01_AE and failing first-line nevirapine and efavirenz-based regimens. Antivir Ther. 2009;14:A155.
19. Schöller-Gyüre M, Kakuda TN, De Smedt G, et al. Pharmacokinetics of TMC125 in HIV-negative volunteers with mild or moderate hepatic impairment. 47th Interscience Conference on Antimicrobial Agents and Chemotherapy, Chicago, IL, September 17–20, 2007. Poster A 1428.
20. Lalezari J, DeJesus E, Osiyemi O, et al. Pharmacokinetics of once-daily etravirine (ETR) without and with once-daily darunavir/ritonavir in antiretroviral-naïve HIV-1 infected adults. 9th International Congress on Drug Therapy in HIV Infection, Glasgow, Scotland, November 9-13, 2008. Abstract O413.
21. Gruzdev B, Rakhmanova A, Doubovskaya E, et al. A randomized, double-blind, placebo-controlled trial of TMC125 as 7-day monotherapy in antiretroviral naive, HIV-1 infected subjects. AIDS. 2003;17:2487–2494.
22. Schöller-Gyüre M, Kakuda TN, Van Solingen-Ristea RM, et al. Bioavailability of the 100 mg etravirine tablet dispersed in water and of the 25 mg pediatric tablet formulation. I 17th IAS, Mexico City, Mexico, 2008. Abstract MOPE0184.
23. Kakuda TN, Königs C, Feiterna-Sperling C, et al. Pharmacokinetics of the next-generation NNRTI etravirine (ETR; TMC125) in HIV-infected children between 6 and 17 years, inclusive. 15th Conference on Retroviruses and Opportunistic Infections, Boston, MA, February 3-6, 2008. Abstract 578.
24. Viganò A, Meroni L, Marchetti G, et al. Successful rescue therapy with a darunavir/ritonavir and etravirine antiretroviral regimen in a child with vertically acquired multidrug-resistant HIV-1. Antivir Ther. 2008;13:839–843.
25. Furco A, Gosrani B, Nicholas S, et al. Successful use of darunavir, etravirine, enfuvirtide and tenofovir/emtricitabine in pregnant woman with multiclass HIV resistance. AIDS. 2009;23:434–435.
26. Izurieta P, Kakuda TN, Clark A, Feys C, Witek J. Safety and pharmacokinetics of etravirine in pregnant HIV-infected women. 12th European AIDS Conference, Cologne, Germany, November 11-14, 2009. Abstract PE 4.1/6.
27. Giguère P, la Porte C, Zhang G, Cameron B. Pharmacokinetics of darunavir, etravirine and raltegravir in an HIV-infected patient on haemodialysis. AIDS. 2009;23:740–742.
28. Aboud M, Castelino S, Back D, Kulasegaram R. Etravirine plasma levels in a patient with decompensated liver disease. AIDS. 2009;23:1293–1295.
29. Montaner J, Yeni P, Clumeck NN, et al; TMC125-C203 Study Group. Safety, tolerability, and preliminary efficacy of 48 weeks of etravirine therapy in a phase IIb dose-ranging study involving treatment-experienced patients with HIV-1 infection. Clin Infect Dis. 2008;47:969–978.
30. TMC125-C223 Writing Group, Nadler JP, Berger DS, et al. Efficacy and safety of etravirine (TMC125) in patients with highly resistant HIV-1: primary 24-week analysis. AIDS. 2007;21:F1–F10.
31. Ruxrungtham K, Pedro RJ, Latiff GH, et al; TMC125-C227 study group. Impact of reverse transcriptase resistance on the efficacy of TMC125 (etravirine) with two nucleoside reverse transcriptase inhibitors in protease inhibitor-naïve, nonnucleoside reverse transcriptase inhibitor-experienced patients: study TMC125-C227. HIV Med. 2008;9:883–896.
32. Yazdanpanah Y, Fagard C, Descamps D, et al; ANRS 139 TRIO Trial Group. High rate of virologic suppression with raltegravir plus etravirine and darunavir/ritonavir among treatment-experienced patients infected with multidrug-resistant HIV: results of the ANRS 139 TRIO trial. Clin Infect Dis. 2009;49:1441–1449.
33. Lazzarin A, Campbell T, Clotet B, et al; DUET-2 study group. Efficacy and safety of TMC125 (etravirine) in treatment-experienced HIV-1-infected patients in DUET-2: 24-week results from a randomised, double-blind, placebo-controlled trial. Lancet. 2007;370:39–48.
34. Madruga JV, Cahn P, Grinsztejn B, et al; DUET-1 study group. Efficacy and safety of TMC125 (etravirine) in treatment-experienced HIV-1-infected patients in 35. DUET-1: 24-week results from a randomised, double-blind, placebo-controlled trial. Lancet. 2007;370:29–38.
35. Katlama C, Haubrich R, Lalezari J, et al; DUET-1, DUET-2 study groups. Efficacy and safety of etravirine in treatment-experienced, HIV-1 patients: pooled 48 week analysis of two randomized, controlled trials. AIDS. 2009;23:2289–2300.
36. Towner W, Lalezari J, Sension MG, et al. Efficacy, safety, and tolerability of etravirine with and without darunavir/ritonavir or raltegravir in treatment-experienced patients: analysis of the etravirine early access program in the United States. J Acquir Immune Defic Syndr. 2010 Feb 3 [Epub ahead of print].
37. Loutfy M, Ribera E, Florence E, et al. Sustained HIV RNA suppression after switching from enfuvirtide to etravirine in the early access programme. J Antimicrob Chemother. 2009;64:1341–1344.
38. Imaz A, del Saz SV, Ribas MA, et al. Raltegravir, etravirine, and ritonavir-boosted darunavir: A safe and successful rescue regimen for multidrug-resistant HIV-1 infection. JAcquir Immune Defic Syndr. 2009;52;382–386.
39. Peeters M, Janssen K, Kakuda TN, et al. Etravirine has no effect on QT and corrected QT interval in HIV-negative volunteers. Ann Pharmacother. 2008;42:757–765.
40. Raoof A, Lachau-Durand S, Verbeeck J, Bailey G, Martens M. Etravirine (TMC125; ETR) has no effect on fetal development in rats and rabbits. 17th International AIDS Conference, Mexico City, Mexico, August 3-8, 2008. Poster TUPE0013.
41. Boffito M, Winston A, Jackson A, et al. Pharmacokinetics and antiretroviral response to darunavir/ritonavir and etravirine combination in patients with high-level viral resistance. AIDS. 2007;21:1449–1455.
42. Anderson MS, Kakuda TN, Hanley W, et al. Minimal pharmacokinetic interaction between the human immunodeficiency virus nonnucleoside reverse transcriptase inhibitor etravirine and the integrase inhibitor raltegravir in healthy subjects. Antimicrob Agents Chemother. 2008;52:4228–4232.
43. Kakuda TN, Schöller-Gyüre M, De Smedt G, et al. Assessment of the steady-state pharmacokinetic interaction between etravirine administered as two different formulations and tenofovir disoproxil fumerate in healthy volunteers. HIV Med. 2009;10:173–181.
44. Schöller-Gyüre M, Kakuda TN, Witek J, et al. Pharmacokinetic interaction between etravirine and lopinavir/ritonavir in HIV-negative volunteers. 12th European AIDS Conference, Cologne, Germany, November 11-14, 2009. Abstract PE4.3/1.
45. Israel D, Kakuda TN, Schöller-Gyüre M, et al. TMC 125 in combination with medications commonly used in HIV infection: summary of drug-drug interactions. American Conference for the Treatment of HIV (ACTHIV) 2007, Dallas, Texas, May 31-June 3, 2007. Poster S3–8.
46. Ménard A, Solas C, Mokthari S, et al. Etravirine-raltegravir, a marked interaction in HIV-1 infected patients: about four cases. AIDS. 2009;23:869–871.
47. Schöller-Gyüre M, Kakuda TN, Woodfall B, et al. Effect of steady state etravirine on the pharmacokinetics and pharmacodynamics of ethinylestradiol and norethindrone. Contraception. 2009;80:44–52.
48. Schöller-Gyüre M, Kakuda TN, De Smedt G, et al. A pharmacokinetic study of etravirine (TMC125) co-administered with ranitidine and omeprazole in HIV-negative volunteers. Br J Clin Pharmacol. 2008;66:508–516.
49. Schöller-Gyüre M, van den Brink W, Kakuda TN, et al. Pharmacokinetic and pharmacodynamic study of concomitant administration of methadone and TMC125 in HIV-negative volunteers. J Clin Pharmacol. 2008;48:322–329.
50. Schöller-Gyüre M, Kakuda TN, Van Solingen-Ristea RM, et al. No clinically relevant effect of etravirine (ETR; TMC125) on digoxin pharmacokinetics in HIV-negative volunteers. 9th International Workshop on Clinical Pharmacology of HIV Therapy, New Orleans, LA, April 7-9 2008. Poster P22.


Coalition promotes important acetaminophen dosing reminders
November 18th 2014It may come as a surprise that each year Americans catch approximately 1 billion colds, and the Centers for Disease Control and Prevention estimates that as many as 20% get the flu. This cold and flu season, 7 in 10 patients will reach for an over-the-counter (OTC) medicine to treat their coughs, stuffy noses, and sniffles. It’s an important time of the year to remind patients to double check their medicine labels so they don’t double up on medicines containing acetaminophen.
Support consumer access to specialty medications through value-based insurance design
June 30th 2014The driving force behind consumer cost-sharing provisions for specialty medications is the acquisition cost and not clinical value. This appears to be true for almost all public and private health plans, says a new report from researchers at the University of Michigan Center for Value-Based Insurance Design (V-BID Center) and the National Pharmaceutical Council (NPC).
Management of antipsychotic medication polypharmacy
June 13th 2013Within our healthcare-driven society, the increase in the identification and diagnosis of mental illnesses has led to a proportional increase in the prescribing of psychotropic medications. The prevalence of mental illnesses and subsequent treatment approaches may employ monotherapy as first-line treatment, but in many cases the use of combination of therapy can occur, leading to polypharmacy.1 Polypharmacy can be defined in several ways but it generally recognized as the use of multiple medications by one patient and the most common definition is the concurrent use of five more medications. The presence of polyharmacy has the potential to contribute to non-compliance, drug-drug interactions, medication errors, adverse events, or poor quality of life.
Medical innovation improves outcomes
June 12th 2013I have been diagnosed with stage 4 cancer of the pancreas, a disease that’s long been considered not just incurable, but almost impossible to treat-a recalcitrant disease that some practitioners feel has given oncology a bad name. I was told my life would be measured in weeks.

