
- Safety & Recalls
- Regulatory Updates
- Drug Coverage
- COPD
- Cardiovascular
- Obstetrics-Gynecology & Women's Health
- Ophthalmology
- Clinical Pharmacology
- Pediatrics
- Urology
- Pharmacy
- Idiopathic Pulmonary Fibrosis
- Diabetes and Endocrinology
- Allergy, Immunology, and ENT
- Musculoskeletal/Rheumatology
- Respiratory
- Psychiatry and Behavioral Health
- Dermatology
- Oncology
FDA advisory panel weighs safety of drug-eluting stents
When used for their approved indications, drug-eluting stents (DES) probably do not increase the risk of death or myocardial infarction (MI) compared with bare metal stents (BMS), an FDA advisory panel concluded at a meeting in Gaithersburg, Md, last month.
When used for their approved indications, drug-eluting stents (DES) probably do not increase the risk of death or myocardial infarction (MI) compared with bare metal stents (BMS), an FDA advisory panel concluded at a meeting in Gaithersburg, Md, last month.
The propensity of DES to increase the risk of stent thrombosis compared with BMS is uncertain, although many of the invited consultants at this meeting of the Circulatory System Devices Panel said they believed that the increased risk of stent thrombosis with DES is real but small compared with BMS.
Perhaps more important are the uncertain but potentially increased risks of stent thrombosis, death, and MI when DES are used in an off-label manner, according to the advisory panel. Instances of off-label use account for at least 60% of total DES use, and this figure could be as high as 75%.
Data from a variety of randomized, controlled trials and registries presented to the panel offered conflicting information about the benefit:risk ratio with DES. Providing much of the safety reassurance were follow-up data from randomized, controlled trials conducted by Boston Scientific and Cordis Corporation, manufacturers of the paclitaxel-eluting stent (PES) and sirolimus-eluting stent (SES), respectively, the 2 DES approved by FDA for use in the United States.
ON-LABEL USE
Data from 4 double-blind, controlled, randomized SES trials, which included 1,748 randomized patients, demonstrated that the rate of stent thrombosis remained in the "low single digit percentages" at 4 years after stent implantation, said Campbell Rogers, MD, chief technology officer, Cordis Corporation. The rate varied among trials according to the definition of stent thrombosis used.
Compared with BMS, the risk of death with the SES was increased by a nonsignificant 28% (6.8% vs 5.3%) and the risk of MI was increased by 3.2% (6.3% to 6.5%). One trial demonstrated a higher rate of noncardiac mortality with the SES, which was not consistent with the other 3 trials.
In patients with diabetes, the SES was associated with a mortality of 11.3% compared with a mortality of 4.3% in patients with diabetes who received BMS. The 4.3% mortality rate in the patients with diabetes subgroup who received the BMS was unusually low, and probably represents an "anomalous finding," Dr Rogers stated.
When any definition of stent thrombosis was used (either "definite," "probable," or "possible," according to Academic Research Consortium [ARC] standards) the rates of stent thrombosis were 3.6% with the SES and 3.3% with the BMS, said Laura Mauri, MD, MSc, chief scientific officer, Harvard Clinical Research Institute, Cambridge, Mass.
The rate of death following stent thrombosis is approximately 30% whether it occurs with the BMS or SES, she noted, and represents a small portion of the deaths in the clinical trials. "Ten percent of deaths are attributable to stent thrombosis," she said.



The possibility of late increases in stent thrombosis, death, and MI with DES over BMS came to the forefront at the 2006 World Congress of Cardiology (WCC) in Barcelona, Spain, where 2 meta-analyses of the SES and PES randomized trials were presented. Results from the BASKET-LATE (Basel Stent Kosten Effektivitäts Trial-Late Thrombotic Events) study also demonstrated an excess of cardiac death and nonfatal MI starting at Month 7 in patients randomized to DES versus BMS. Finally, 3-year follow-up data of 8,146 patients who received DES demonstrated an increasing incidence of stent thrombosis with time, at a rate of 0.6% per year. It was these data that set in motion the convening of the FDA advisory panel.
A new meta-analysis of the SES and PES trials presented by Gregg Stone, MD, director of research and education for the Center for Interventional Vascular Therapy at Columbia University Medical Center, New York, NY, demonstrated, however, that an excess of stent thrombosis in the DES arms did not translate into an increase in clinical events. He explained that the discordant finding compared with the meta-analyses presented in Barcelona was the result of more complete data capture. The presenters at WCC included follow-up data gathered from abstracts and Internet sources for their data analysis. (At WCC, the authors of the 2 pivotal meta-analyses lamented the difficulty in obtaining long-term follow-up data).

Nevertheless, Dr Topol wondered why the small increased risk of stent thrombosis did not translate into higher rates of MI and mortality in the DES arms. "There seems to be a disconnect...why is there a lack of linkage between stent thrombosis and events?" he asked.
Drs Stone and Rogers answered that the reduction in restenosis with DES is responsible for the disconnect. "Restenosis is not cosmetic....there are deaths from repeat procedures," Dr Rogers said.

Another consultant to the FDA advisory panel, Steven Nissen, MD, chief of cardiology at the Cleveland Clinic, Cleveland, Ohio, noted that few patients in the randomized clinical trials were followed to 4 or 5 years, and he raised the question of whether an accumulation of late events will overwhelm the early benefit with DES. Because the artery never re-endothelializes with DES, "nothing to me suggests that the problem goes away," he said. "In the long run, [patients] may be worse off."
OFF-LABEL USE
Examination of off-label data related to DES was even more precarious, with reliance on uncontrolled registries.
Dr Baim presented data from the 7,000-patient ARRIVE I and ARRIVE II registries of real-world experience with the PES, including patients with complex lesions and those with multiple stents. As expected, the death rate in PES recipients with more complex lesions was higher than the death rate in PES recipients with simple lesions.
Despite the higher death rate in the more complex patients, this rate was comparable to that of alternative forms of revascularization, such as coronary artery bypass graft (CABG) surgery, Dr Baim said. That contention drew criticism from Norman S. Kato, MD, a consultant to the panel, and cardiothoracic surgeon from Cardiac Care Medical Group, Encino, Calif, who noted that the 6.5% mortality rate for CABG quoted by Dr Baim was outdated. "The historical CABG mortality is not 6.5%," he said. According to Dr Kato, a more realistic figure for CABG mortality is about 2% at 2 years.
The superiority of CABG over percutaneous coronary intervention (PCI) and stenting for multivessel disease was supported by 2 presenting surgeons, Peter Smith, MD, chief of the department of surgery at Duke University, Durham, NC, and Robert Guyton, MD, chief of cardiothoracic surgery at Emory University, Atlanta, Ga. Dr Guyton said that in the Stent or Surgery Trial of 988 patients with multivessel coronary disease, mortality rates at 2 years were 2% in the CABG arm and 5% in the PCI arm, a difference that increased out to 5-year follow-up.
"An off-label extension of DES does not meet the need of our patients," Dr Smith said.
Data on DES from a Swedish registry of approximately 60,000 patients with DES or BMS impressed many of the consultants and the FDA advisory panel. Lars Wallentin, MD, PhD, professor of cardiology and head, Uppsala Clinical Research Center, Sweden, said that compared with BMS, "the trend over time is to higher mortality with the DES group." He noted that after the first 6 months, the relative risk of mortality with DES increased by 32%, and that the "pattern is the same with MI," although the difference was not significant.
Even in patients with 1 stent implanted, "there is a significant early hazard in the BMS group and a late hazard in the DES group," Dr Wallentin said. The increased risk of clinical events in the DES arms increased linearly, he said.
The Swedish registry of both on-label and off-label use is of sufficient size to detect small differences in event rates between DES and BMS, said Robert Harrington, MD, citing the 0.5% per year excess risk with DES. Dr Harrington is a consultant to the FDA panel, and director of cardiovascular clinical trials at the Duke Clinical Research Institute, Durham, NC,
"DES has created a new entity- some would even say a new monster-in stent thrombosis," Dr Topol said. "The late thrombosis may well be associated with an increase of death and MI in 'off-label' patients." The most important message is that significant uncertainties exist with off-label use of DES, he said.
Other consultants and panelists agreed that the benefit:risk ratio may not favor the use of DES in off-label settings.
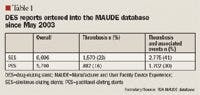
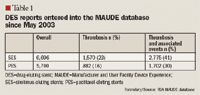
PASSIVE SURVEILLANCE




THE IMPORTANCE OF DUAL ANTIPLATELET THERAPY
A separate discussion involved the optimal duration of antiplatelet therapy for patients with DES. Again, the data varied according to the study or the registry, with some data sets demonstrating that extended durations of dual antiplatelet therapy (clopidogrel and aspirin) lowered the risk of stent thrombosis and clinical events, whereas others demonstrated no increase in risk beyond 6 months of dual antiplatelet therapy.



The BASKET-LATE investigators followed 746 of their patients 1 year after discontinuation of clopidogrel (patients with DES in the randomized trial were on dual antiplatelet therapy for 6 months). The rate of death/MI between Months 7 and 18 was 4.9% after DES versus 1.3% after BMS. The DES group maintained a lower rate of target vessel revascularization (TVR) compared with the BMS group at 18 months.

In listening to the second day of testimony, Sidney Smith, MD, professor of medicine at the University of North Carolina in Chapel Hill, NC, who was representing the AHA, said: "It looks like we got it right" with the 12-month recommendation.
The importance of adhering to antiplatelet recommendations should be emphasized in package inserts or other FDA-provided information for patients and physicians, the advisory panel agreed. This approach was supported by Gregory J. Dehmer, MD, president of SCAI: "It is strongly recommended that all patients receive counseling about the importance of continuing dual antiplatelet therapy both before and after stent placement, and that there be greater education provided for all healthcare workers about the need for this therapy."
Dr Topol also suggested that genomic studies would identify patients who may need extended antiplatelet therapy.
BOTTOM LINE
One certain conclusion made at the meeting is that when used outside of the indicated patient populations, DES are associated with an increased risk of stent thrombosis, death, and MI compared with on-label use, and the same is true of BMS, said William H. Maisel, MD, MPH, from Beth Israel Deaconess Medical Center in Boston, Mass, and chair of the FDA advisory panel.
"Importantly, there is no increased risk of death or MI when DES are used on-label," he stated. "The panel would like to see the amount of off-label use go down." Such a decrease would include less use of DES for bifurcation lesions and lesions that already are thrombus-laden, he said.
Most of the consultants called for more judicious and selective off-label use of DES until further data are available. "Any application off-label should give someone pause, because we don't know if [patients] are benefiting," said Clyde Yancy, MD, FDA advisory panel member, and director of the congestive heart failure/transplant program, University of Texas Southwestern Medical Center, Dallas, Tex.
LITERATURE CITED
The following is a listing of the literature cited by the FDA advisory panel for its December 7 and 8, 2006, meeting in Gaithersburg, Md.
1. Berlin JA, Santanna J, Schmid CH, Szczech LA, Feldman HI; Anti-lymphocyte Antibody Induction Therapy Study Group. Individual patient- versus group-level data meta-regressions for the investigation of treatment effect modifiers: Ecological bias rears its ugly head. Stat Med. 2002;21:371–387.
2. Bossi I, Klersy C, Black AJ, et al. In-stent restenosis: long-term outcome and predictors of subsequent target lesion revascularization after repeat balloon angioplasty. J Am Coll Cardiol. 2000;35:1569–1576.
3. Chen MS, John JM, Chew DP, Lee DS, Ellis SG, Bhatt DL. Bare metal stent restenosis is not a benign clinical entity. Am Heart J. 2006;151:1260–1264.
4. Cutlip DE, Baim DS, Ho KK, et al. Stent thrombosis in the modern era: A pooled analysis of multicenter coronary stent clinical trials. Circulation. 2001;103:1967–1971.
5. Dorsam RT, Kunapuli SP. Central role of the P2Y12 receptor in platelet activation. J Clin Invest. 2004;113:340–345.
6. Farb A, Sangiorgi G, Carter AJ, et al. Pathology of acute and chronic coronary stenting in humans. Circulation. 1999;99:44–52.
7. Farb A, Weber DK, Kolodgie FD, Burke AP, Virmani R. Morphological predictors of restenosis after coronary stenting in humans. Circulation. 2002;105:2974–2980.
8. Farb A, Burke AP, Kolodgie FD, Virmani R. Pathological mechanisms of fatal late coronary stent thrombosis in humans. Circulation. 2003;108:1701–1706.
9. Gurbel PA, Bliden KP, Samara W, et al. Clopidogrel effect on platelet reactivity in patients with stent thrombosis: results of the CREST study. J Am Coll Cardiol. 2005;46:1827–1832.
10. Heller LI, Shemwell KC, Hug K. Late stent thrombosis in the absence of prior intracoronary brachytherapy. Catheter Cardiovasc Interv. 2001;53:23–28.
11. Hoye A, Iakovou I, Ge L, et al. Long-term outcomes after stenting of bifurcation lesions with the "crush" technique. J Am Coll Cardiol. 2006;47:1949–1958.
12. Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA. 2005;293:2126–2130.
13. Joner M, Finn AV, Farb A, et al. Pathology of drug-eluting stents in humans: Delayed healing and late thrombotic risk. J Am Coll Cardiol. 2006;48:193–202.
14. Kaiser C, Brunner-La Rocca HP, Buser PT, et al; BASKET Investigators. Incremental cost-effectiveness of drug-eluting stents compared with a third-generation bare-metal stent in a real-world setting: Randomised Basel Stent Kosten Effektivitäts Trial (BASKET) [erratum in Lancet. 2005; 366:2086]. Lancet. 2005;366:921–929.
15. Katayama T, Nakashima H, Takagi C, et al. Predictors of sub-acute stent thrombosis in acute myocardial infarction patients following primary coronary stenting with bare metal stent. Circ J. 2006;70:151–155.
16. Tung R, Kaul S, Diamond GA, Shah PK. Narrative review: Drug-eluting stents for the management of restenosis: A critical appraisal of the evidence. Ann Intern Med. 2006;144:913–919.
17. Kuchulakanti P, Chu WW, Torguson R, et al. Correlates and long-term outcomes of angiographically proven stent thrombosis with sirolimus- and paclitaxel-eluting stents. Circulation. 2006;113:1108–1113.
18. Moreno R, Fernandez C, Hernandez R, et al. Drug-eluting stent thrombosis: Results from a pooled analysis including 10 randomized studies. J Am Coll Cardiol. 2005;45:954–959.
19. Moses J, Leon MB, Popma JJ, et al; SIRIUS Investigators. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med. 2003;349:1315–1323.
20. Muni N, Gross TP. Problems with drug-eluting coronary stents-the FDA perspective. N Engl J Med. 2004;351:1593–1595.
21. Nayak AK, Kawamura A, Nesto RW, et al. Myocardial infarction as a presentation of clinical in-stent restenosis. Circ J. 2006;70:1026–1029.
22. Nordmann AJ, Briel M, Bucher HC. Mortality in randomized controlled trials comparing drug-eluting vs. bare metal stents in coronary artery disease: A meta-analysis. Eur Heart J. 2006;27:2784–2814.
23. Ong AT, McFadden EP, Regar E, de Jaegere PP, van Domburg RT, Serruys PW. Late angiographic stent thrombosis (LAST) events with drug-eluting stents. J Am Coll Cardiol. 2005;45:2088–2092.
24. Ong AT, Hoye A, Aoki J, et al. Thirty-day incidence and six-month clinical outcome of thrombotic stent occlusion after bare-metal, sirolimus, or paclitaxel stent implantation. J Am Coll Cardiol. 2005;45:947–953.
25. Pfisterer M, Brunner- La Rocca HP, Buser PT, et al; for the BASKET-LATE Investigators. Late clinical events after clopidogrel discontinuation may limit the benefit of drug-eluting stents. J Am Coll Cardiol. 2006;48:2584–2591.
26. Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines; American College of Cardiology/American Heart Association/Society for Cardiovascular Angiography and Interventions Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention. ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention-summary article. Circulation. 2006;113:156–175.
27. Spertus JA, Kettelkamp R, Vance C, et al. Prevalence, predictors, and outcomes of premature discontinuation of thienopyridine therapy after drug-eluting stent placement: Results from the PREMIER registry. Circulation. 2006;113:2803–2809.
28. Stone GW, Ellis SG, Cox DA, et al; TAXUS-IV Investigators. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med. 2004;350:221–231.
29. Virmani R, Guagliumi G, Farb A, et al. Localized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: Should we be cautious? Circulation. 2004;109:701–705.
30. Walters DL, Harding SA, Walsh CR, Wong P, Pomerantsev E, Jang IK. Acute coronary syndrome is a common clinical presentation of in-stent restenosis. Am J Cardiol. 2002;89:491–494.
31. Wang F, Stouffer GA, Waxman S, Uretsky BF. Late coronary stent thrombosis: Early vs. late stent thrombosis in the stent era. Catheter Cardiovasc Interv. 2002;55:142–147.
32. Williams DO, Abbott JD, Kip KE; DEScover Investigators. Outcomes of 6906 patients undergoing percutaneous coronary intervention in the era of drug-eluting stents: Report of the DEScover Registry. Circulation. 2006;114:2154–2162.
33. Wiviott SD, Antman EM. Clopidogrel resistance: A new chapter in a fast-moving story. Circulation. 2004;109:3064–3067.

FDA Approves Combination Therapy for Pulmonary Arterial Hypertension
March 25th 2024J&J’s Opsynvi is single-tablet combination of macitentan, an endothelin receptor antagonist, and tadalafil, a PDE5 inhibitor. It will be priced on parity with Opsumit, which is also a J&J product to treat patients with PAH.




FDA Issues Complete Response Letter for Onpattro in Heart Failure Indication
October 9th 2023Alnylam Pharmaceuticals will no longer pursue this indication of Onpattro and will instead on focus on a label expansion for Amvuttra, which is in phase 3 development to treat patients with cardiomyopathy of ATTR amyloidosis.


