
- Safety & Recalls
- Regulatory Updates
- Drug Coverage
- COPD
- Cardiovascular
- Obstetrics-Gynecology & Women's Health
- Ophthalmology
- Clinical Pharmacology
- Pediatrics
- Urology
- Pharmacy
- Idiopathic Pulmonary Fibrosis
- Diabetes and Endocrinology
- Allergy, Immunology, and ENT
- Musculoskeletal/Rheumatology
- Respiratory
- Psychiatry and Behavioral Health
- Dermatology
- Oncology
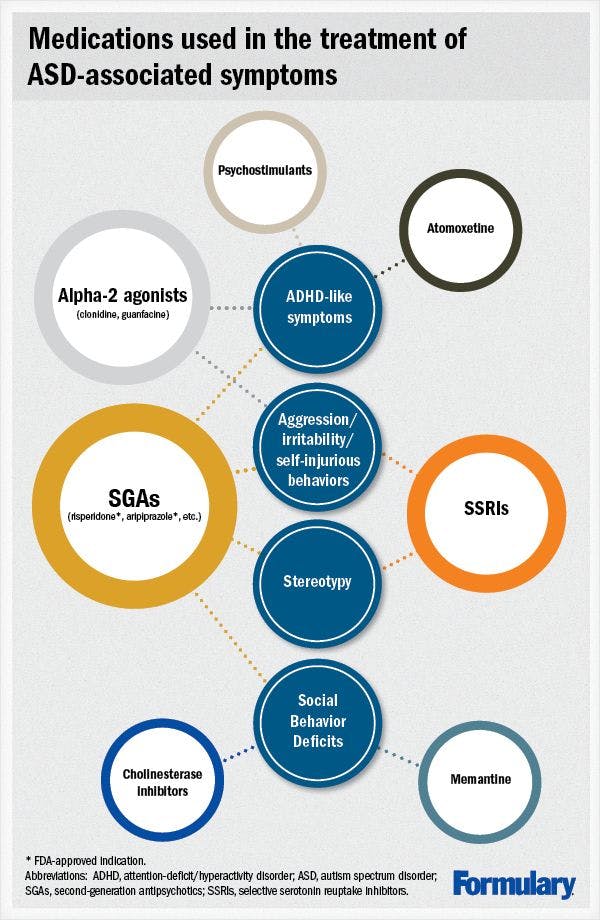
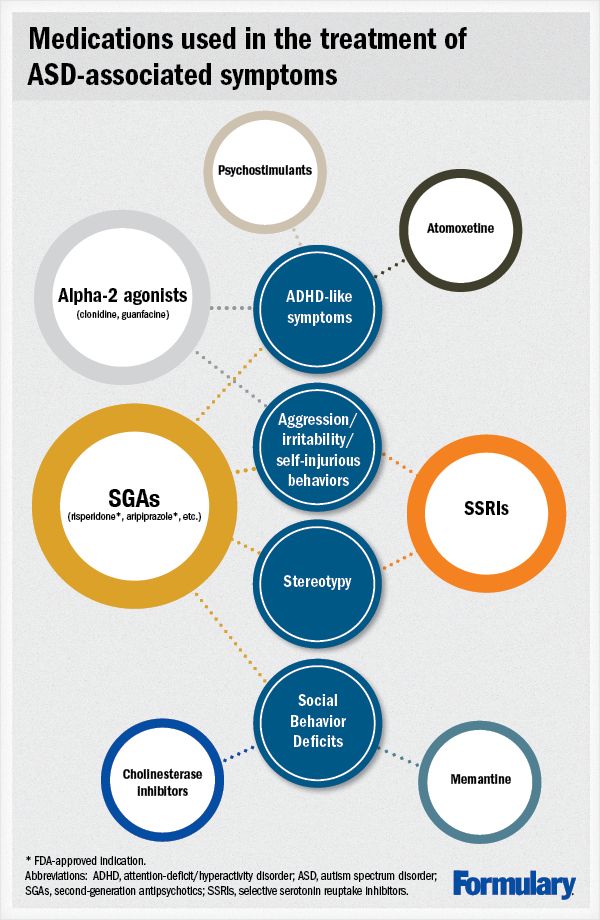
[INFOGRAPHIC] Medication use in autism spectrum disorders: What is the evidence?
Autism spectrum disorders (ASD) are complex neurodevelopmental disorders that involve significant social functional impairment and behavioral inflexibility. Autism is the most severe form of ASD and includes significant impairment in communication skills. Treatment of ASD is complex and involves a comprehensive educational interventional plan. Medications are used only as adjuncts, and only in cases in which maladaptive behaviors are severe or life-threatening, or to enable a patient to participate in their behavioral therapies. The most commonly used medications include second-generation antipsychotics (SGAs), selective serotonin reuptake inhibitors (SSRIs), and psychostimulants. Risperidone and aripiprazole are the only medications to carry an FDA indication to treat ASD-related symptoms. There is interest in using newer agents, such as atomoxetine, galantamine, rivastigmine, and memantine, to treat ASD-associated symptoms, but data are lacking to support their use.
ABSTRACT
Autism spectrum disorders (ASD) are complex neurodevelopmental disorders that involve significant social functional impairment and behavioral inflexibility. Autism is the most severe form of ASD and includes significant impairment in communication skills. Treatment of ASD is complex and involves a comprehensive educational interventional plan. Medications are used only as adjuncts, and only in cases in which maladaptive behaviors are severe or life-threatening, or to enable a patient to participate in their behavioral therapies. The most commonly used medications include second-generation antipsychotics (SGAs), selective serotonin reuptake inhibitors (SSRIs), and psychostimulants. Risperidone and aripiprazole are the only medications to carry an FDA indication to treat ASD-related symptoms. There is interest in using newer agents, such as atomoxetine, galantamine, rivastigmine, and memantine, to treat ASD-associated symptoms, but data are lacking to support their use.
Autism spectrum disorders (ASD) are neurodevelopmental conditions that develop in early childhood that involve both impairment in social function and behavioral inflexibility. The class encompasses 3 disorders: “classic” autism, Asperger’s disorder, and pervasive developmental disorder not otherwise specified (PDD NOS).The latter is given to patients whose symptoms do not meet the criteria for either autism or Asperger’s disorder. Patients who have an intelligence quotient >70 and who began speaking at the expected age are diagnosed with Asperger’s disorder.1 Autism is the most severe form of the 3 and involves substantial deficits in 3 areas: 1) social interaction, 2) communication skills (including delay in speech development), and 3) behavioral and cognitive inflexibility. Patients with autism are unable to use nonverbal cues such as eye-to-eye contact or gestures to communicate and cannot “connect” socially with others. About half are nonverbal or have grossly impaired speech. Behavioral inflexibility manifests as repetitive and restricted behavior, activities, or interests. The presence of repetitive, nonfunctional, and atypical behaviors is known as “stereotypy.” Examples of these activities include perseveration, rocking, hand flapping, finger movements, or hair twirling.1,2
No single pathognomonic feature identifies ASD in children. Social deficits occur early, but are subtle and can be difficult to recognize. The most distinguishing feature appears to be delayed or absent joint attention, a phenomenon in normal children in which they show enjoyment in sharing an object or experience with another by looking back and forth between the two. Delay in speech development is considered a hallmark, because this is the symptom that parents first recognize as abnormal. This usually occurs at age 15 to 18 months, although treatment is not usually sought until several months later.2
Patients with autism have a high incidence of comorbid conditions. Approximately 70% have comorbid mental retardation, and a third will have at least 2 seizures by the time they reach late adolescence. Sleep disturbances and gastrointestinal symptoms are also common. Patients with autism are not usually capable of living independently.1
EPIDEMIOLOGY
The wide variation in symptoms in a child can make diagnosis difficult. ASD is more prevalent than once believed. According to the Centers for Disease Control and Prevention, 1 in 88 children carried an ASD diagnosis in 2008. This represents a 78% increase since 2002. This increase may be due in part to heightened public awareness of the condition and the resulting increase in diagnosis. More cases are being diagnosed at an earlier age (before 3 years), but most are not diagnosed under after aged 4 years. Within the spectrum, autism is diagnosed in 44% of cases, ASD/PDD NOD in 47%, and Asperger’s in 9%. Of the 3 diagnoses, Asperger’s has the longest delay in diagnosis (75 months vs. 48 months for autism). ASD is 5 times more common in boys than girls.3
ETIOLOGY
The exact etiology of autism is unknown. ASD has a high degree of heritability that is complex and involves multiple genes. The phenotypic manifestation of these genes is highly variable, complicating the search for a cause. Although the majority of ASD cases result from genetics, environmental triggers may contribute. Many of the brain abnormalities associated with ASD occur during the first and second trimesters of pregnancy. Environmental factors may play a role, including exposure to teratogens. Although attempts have been made to link ASD to postnatal exposures to the measles, mumps, and rubella (MMR) vaccine and mercury-containing vaccines, no association has ever been proved. The original study attempting to link MMR to autism published by Wakefield in The Lancet in 1998 has been discredited, and the majority of the authors who published the study with Wakefield retracted their findings. Numerous reports published since the original proposals have refuted the link of autism with either MMR or mercury-containing vaccines.2,4
SCREENING AND DIAGNOSIS
The Diagnostic and Statistical Manual of Mental Disorders IV Text Revision (DSM-IV-TR) contains diagnostic criteria for autism, Asperger’s disorder, and PDD NOS. Multiple tools exist for screening, diagnosing, and assessing ASD. A commonly used tool to monitor outcomes in clinical trials is the Aberrant Behavior Checklist (ABC). It was originally developed to measure problem behaviors in the developmentally delayed population but has also been validated for use in the ASD population. It contains 58 items and 5 subscales (Table 1). Each item is rated by the patient’s caregiver (such as family or a teacher) on a 4-point scale, from 0 (“not at all a problem”) to 3 (“the problem is severe in degree”). There is no composite ABC scale; each subscale is scored separately. Trial outcomes are designed around specific subscales.5,6
Table 1. Aberrant Behavior Checklist (ABC)*
Subscale
No. of items
Possible maximum score
Irritability, agitation, crying
15
45
Lethargy/social withdrawal
16
48
Stereotypic behavior
7
21
Hyperactivity/noncompliance
16
48
Inappropriate speech
4
12
* Please refer to the text for a description of the ABC.
TREATMENTS
ASD is not curable and thus must be managed as a chronic condition. The primary goals are to minimize the core deficits and maximize independent functioning and quality of life for both the patient and their family. Educational interventions are the cornerstones of treatment. These usually involve behavioral and rehabilitative components that address the complex deficits that exist with autism. The components can involve occupational therapies, behavior modification, and speech and language therapies.7
Patients with ASD experience a wide range of behavioral dysfunctions that influence their physical health and relationships. These dysfunctions can also interfere with educational interventions. Although usually harmless, stereotypy can prevent or distract a patient with autism from learning a new skill or accomplishing a task. It can also be self-injurious if it involves such activities as head banging or picking at skin. Attempts to distract the patient from stereotypical behaviors can cause distress that can escalate to aggression, self-injurious behaviors, and temper tantrums. If severe enough, these behaviors can be dangerous to patients or their caregivers. Because many comorbid psychiatric conditions, such as depression and anxiety, can contribute to these behaviors, they should be ruled out. Medical causes of pain or discomfort, such as otitis media or urinary tract infections, should also be ruled out as causes for escalation of maladaptive behaviors.7
Medication should be considered in the treatment of ASD only if nonpharmacologic interventions fail and the maladaptive behaviors are severe. Medications do not treat the core symptoms of ASD, nor can they cure it. Medications are adjuncts, only, that may be used to decrease the severity of symptoms, help patients participate more actively in educational interventions, or help them live outside of institutional settings. Patients with ASD are more sensitive to medication side effects, and so the benefits of use must always be weighed against the risk of developing adverse drug reactions (ADRs).
Although most products are not FDA-approved, medication is used frequently in the treatment of ASD. In a recent survey of 2,853 children in the Autism Treatment Network, 27% were using at least 1 psychotropic medication. Use ranged from 11% in children aged 3 to 5 years to 66% in those aged 12 to 17. Much of the use was related to comorbid psychiatric diagnoses, including attention-deficit/hyperactivity disorder (ADHD)-like symptoms, bipolar disorder, obsessive-compulsive disorder, depression, and anxiety. Stimulants were used in 13% of patients, selective serotonin reuptake inhibitors (SSRIs) and second-generation antipsychotics (SGAs) were each used by 8%, and alpha-2 agonists in 7%.8
Despite the number of medications used to treat symptoms of ASD, very little evidence exists to support the use of most.9 Studies of medications in ASD are sparse, have small sample sizes, and are often open-label. Trials are complicated by concomitant use of other medications to treat ASD-related symptoms. Often investigators have difficulty recruiting enough subjects. Children with ASD are also more sensitive to the side effects of medications. The medications used to treat ASD-related symptoms were chosen based upon their ability to treat similar symptoms in other psychiatric disorders. For example, SSRIs are used to treat stereotypical behavior based upon their use in the treatment of obsessive-compulsive disorder. Most medications used to treat ASD symptoms do not carry an FDA indication for this use. The following sections detail the medications most frequently used to treat ASD-related symptoms. These medications are also summarized in Table 2.

Antipsychotics.
Antipsychotics are the most studied medications in the treatment of ASD. The main use is for associated aggression, irritability, and self-injurious behavior. Antipsychotics can, however, also be used to treat stereotypies and ADHD-like symptoms. Haloperidol is a first-generation antipsychotic that has been used and studied in ASD. An average dose of 1.12 mg/d decreased maladaptive behaviors in 2 clinical trials. Doses exceeding this had no additional effectiveness. Use was associated with a high incidence of side effects, including sedation, paradoxical increases in irritability, and dystonias. At doses of 1.75 mg/d, one-third of patients developed dyskinesias, mostly affecting the face and mouth.10
Of the antipsychotics prescribed to children, over 90% are SGAs. Risperidone is the most studied SGA in ASD, and the most commonly prescribed antipsychotic in pediatric patients. Risperidone and aripiprazole are the only 2 SGAs that carry FDA indications for treating irritability associated with autism in children.
Risperidone has reduced ASD-related maladaptive behaviors in multiple studies. The strongest evidence for the efficacy of risperidone derives from the Research Units on Pediatric Psychopharmacology (RUPP) Autism Network studies. In an 8-week randomized, double-blind, placebo-controlled (RDBPC) trial of 101 children aged 5 to 17 years, a mean risperidone dose of 1.8 mg/d resulted in a 14.9-point decrease in the ABC-irritability (ABC-I) subscale (versus -3.6 points for placebo, P<0.001). Significant decreases in the other 4 ABC subscales also occurred with risperidone treatment. Of the subjects receiving risperidone, 69% were labeled as responders (as defined by a >25% decrease in the ABC-I), versus 12% for placebo (P<0.001). Although 3 children withdrew from the risperidone group for lack of efficacy, none were withdrawn due to ADRs. Weight gain was higher in the risperidone group (2.7±2.9 kg vs 0.8±2.2 kg, P<0.001). The most common side effects were fatigue, drowsiness, and tremor. No other extrapyramidal symptoms (EPS) were reported.11
A 4-month open-label extension of the original 8-week trial enrolled 63 subjects who responded to risperidone during the original trial. The mean risperidone dose was approximately 2 mg/d. A 2.2-point increase in the ABC-I occurred (P=.02), but remained below pretreatment scores. Of the other subscales, only stereotypy showed a minor increase. ADRs were similar to the first trial. Total weight gain over the 6 months was 5.1 kg (+3.6 kg, P<0.001) and was greater than anticipated at the start of the trial. Of the study withdrawals, only 1 occurred due to side effects (constipation). A subsequent 8-week discontinuation phase resulted in a relapse rate of 62.5% in the placebo group. The National Institute of Mental Health (the sponsoring body) ruled that this phase be discontinued immediately.12
Aripiprazole reduced symptoms of irritability in patients with ASD in several small studies. The strongest the evidence for its utility comes from the 2 manufacturer-sponsored trials that led to its approval by the FDA for the treatment of ASD-associated symptoms of irritability. Both were RDBPC 8-week trials in children aged 6 to 17 years. In addition to a DSM-IV-TR ASD diagnosis, patients had to have ASD irritability-type behaviors such as tantrums, aggression, or self-injurious behavior. The first trial involved a flexible dosing schedule starting at 2 mg/d and increasing weekly to a maximum dose of 15 mg/d by 6 weeks at the latest. In 98 patients with a mean age of 9.3 years, the between-group change in ABC-I was -7.9 (CI, -11.7 to -4.1; P<0.001). Significant declines occurred in all other ABC subscales with the exception of lethargy/social withdrawal. Response (defined as a >25% reduction in the ABC-I scale) occurred in 52.2% of patients on aripiprazole (vs 14.3% placebo, P<.001). Side effects occurred in 91.5% of patients on aripiprazole (vs 72% on placebo). The most common side effects were fatigue, somnolence, sedation, drooling, vomiting, diarrhea, and tremor. EPS was reported in 7 cases of patients receiving aripiprazole versus 4 for placebo. None involved either acute dystonias or tardive dyskinesias.13
The second trial involved fixed-dose aripiprazole (5 mg, 10 mg, or 15 mg daily) in 218 patients with a mean age of 9.7 years. Decreases in ABC-I were statistically significant for all doses (vs placebo) in a dose-dependent fashion. In the 5-mg group, the total change was -4.0 (P=.032); for 10 mg, -4.8 (P=.008); and for 15 mg, -6.0 (P=.001). The 15-mg dose produced statistically significant decreases in all other subscales but lethargy/social withdrawal, and all doses produced statistically significant decreases in the stereotypy and hyperactivity subscales. Compared with a 72.5% incidence of side effects in placebo patients, side effects were experienced by 85.2% to 89.8% of patients on aripiprazole (not dose-dependent). ADRs resulted in 17 withdrawals (due to sedation, drooling, and tremor). EPS occurred in 22% to 23% of patients in each group of aripiprazole (vs. 11.8% on placebo), and was limited to tremor and extrapyramidal syndrome. Patients on aripiprazole gained 1.4 to 1.6 kg (vs 0.4 kg on placebo, P< .05).14
Evidence for the use of other SGAs is sparse. Olanzapine and ziprasidone each have 1 clinical trial demonstrating reduced maladaptive behaviors, but sample sizes in both cases were small (<20). In separate small trials, quetiapine has shown mixed results, mostly suboptimal.10,15
Selective serotonin reuptake inhibitors
Because the repetitive and maladaptive behaviors exhibited by patients with ASD resemble those of obsessive-compulsive disorder, treatment with SSRIs is common. Evidence from research has yielded mixed results. One trial of citalopram in 149 children failed to find any benefit.15,16 In early trials, fluvoxamineimproved repetitive behaviors and language usage in 8 of 15 adults, but a subsequent trial failed to find similar responses in children.10 Similarly, a trial of paroxetine in 15 institutionalized patients initially showed benefit on aggression and self-injurious behavior, but the effect dampened after 4 weeks of treatment.17 A small trial of escitalopram in 28 subjects demonstrated improvement in the ABC-irritability subscale.10
Although the total number of patients treated with either is small, both sertraline and fluoxetine have shown the most promise. Sertraline improved aggression and self-injurious behavior in 8 of 9 patients in 1 open-label trial (dosing 25–150 mg/d). A separate open-label trial showed improved response to environmental change in 8 of 9 children (aged 6–12) at doses of 25 to 50 mg/d. 10[J1] In an open-label trial, 57% of patients with ASD (n=42) responded to a mean sertraline dose of 122 mg/d with significant decreases in aggressive and repetitive behaviors. Of note, those with Asperger’s disorder had no response (n=6).18
In an 8-week DBPC crossover study in 34 children aged 5 to 17 years, fluoxetine at mean doses of 0.38 mg/kg/d decreased the 20-point compulsion subscale of the Yale-Brown Obsessive-Compulsive Scale (Y-BOCSc) by 1.55 points (vs 0.25 for placebo; P=.004 to .038 depending on analysis type) with evidence of progressive treatment effects over the treatment period.19 Similarly, a mean fluoxetine dose of 64.75 mg/d decreased the Y-BOCSc by 3.7 points (P=.005) in over 12 weeks in a RDBPC trial involving 37 adult patients with ASD. Fluoxetine was well-tolerated in both trials. Side effects were mild, not statistically different from placebo, and included nightmares or vivid dreams, mild insomnia, dry mouth, and headaches.16
Stimulants and atomoxetine.
The DSM-IV-TR essentially precludes a diagnosis of ADHD if a patient has ASD. However, patients with autism frequently have ADHD-like symptoms, including distractibility, hyperactivity, excitability, and difficulty concentrating. As with ADHD, psychostimulants are considered first-line to treat these symptoms. Unlike children with ADHD, children with ASD are not as responsive to stimulants and have increased sensitivity to side effects such as agitation and emotionality. Methylphenidate is the preferred agent, because it has been used in the bulk of clinical experience and research. Short-acting formulations should be used first in order to gauge tolerability.20
Although a number of trials demonstrated efficacy of methylphenidate in treating ADHD-like symptoms in children with ASD, the strongest evidence to date comes from the RUPP trials. In a 4-week RDBPC crossover trial, 72 children aged 5 to 14 were treated with low-dose (0.125 mg/kg/d), medium-dose (0.25 mg/kg/d), and high-dose (0.5 mg/kg/d) methylphenidate, given in 3 divided doses. During this phase, 49% were found to be responders, and 18% stopped the medication due to intolerance. This phase was also used to find the patient’s “best dose” for response (as measured by the ABC-I) with minimal side effects. During the crossover phase, the ABC-I decreased from 30.9–33.2 to 17.2–20.1 (depending on the evaluator; vs 26 for placebo, P<.001).21 In the second phase, which was an 8-week “open-label” trial of responders (n=34) on their “best dose,” response was maintained. The treatment failed to show benefit on the other ABC subscales. Indeed, the most common side effects included irritability, lethargy, sadness, dullness, and social withdrawal. In a subsequent subanalysis of 33 patients from this study, significant improvement in joint attention, self-regulation, and ability to regulate emotions was detected.22
Two small RDBPC suggest potential minor benefits of atomoxetine in children with ASD with ADHD symptoms. The first trial was a crossover trial that included 16 patients aged 5 to 15 years. Over 6 weeks, 16 patients taking a mean atomoxetine dose of 44.2 + 21.9 mg/d experienced a mean drop of 5 points on the ABC-hyperactivity scale (vs. 0.1 point for placebo, P=.043). There was no correlation between dose and either severity of symptoms or degree of improvement.23 In the second trial, 97 subjects aged 6 to 17 years were randomly assigned to either fixed-dose atomoxetine (1.2 mg/kg/d) or placebo. After 8 weeks, subjects taking atomoxetine experienced a 8.2-point drop in the 54-point ADHD rating scale score (vs 1.2 on placebo, P<.001). Atomoxetine was well tolerated in both trials. Compared with placebo, the most common side effects were nausea, decreased appetite, fatigue, and early morning awakening.24 Both trials were sponsored by the drug manufacturer. Although these trials suggest possible benefit of atomoxetine in the treatment of ASD-associated ADHD-like symptoms, further research is needed before it can be considered as first-line therapy.
Although clonidine and guanfacine have been used to treat symptoms of ADHD, data on their use in ASD is sparse. Both risperidone and aripiprazole have demonstrated a decrease in ADHD-like symptoms in children with ASD. However, because of the risk for weight gain and movement disorders, they are not recommended for use unless the degree of impulsivity threatens the child’s life (eg, dangerous or impulsive running or jumping), or in those children with comorbid irritability or aggression.20
Medications used to treat Alzheimer’s disease.
There has been interest in the use of both cholinesterase inhibitors and the glutamatergic antagonist memantine for improving executive level functional deficits, such as problem-solving, decision-making and social skills, in patients with ASD. The interest stems from autopsy findings that show a deficit of cholinergic receptors and abnormal functioning of those receptors in the cerebral cortex and prefrontal regions of the brain. Trials of these agents have been small and often open-label.25 One RDBPC 10-week trial of 34 patients on donepezil 10 mg/d failed to show any difference in performance on a battery of tests designed to measure cognitive function, including verbal ability and problem-solving.26 Rivastigmine 0.8 mg twice daily improved expressive speech and autistic behaviors (as a 3-point drop in the Childhood Autism Rating Scale score) in one open-label 12-week trial in 32 patients aged 2 to 12 years.25 Galantamine has demonstrated mild improvements in hyperactivity, eye contact, and inappropriate speech, but results are limited to a total of 23 patients.27,28
Additional autopsy findings demonstrate decreased neuronal size in the highly interconnected structures of the limbic system. These findings suggest neuronal immaturity, which affects the ability to form memories. An “excitotoxicity” state may also exist in which persistent activation of N-methyl-D-aspartate (NMDA) receptors leads to high levels of the activating neurotransmitter glutamate and subsequent neuronal death. Small trials of both amantadine, which is structurally related to memantine, and D-cycloserine, which acts as partial agonist at the NMDA receptor, showed positive effects on ASD. These findings led to interest in memantine for treating ASD.29 In 1 8-week open-label trial in 14 subjects aged 3 to 12 years, memantine 0.4 mg/kg (up to 20 mg/d) led to a small improvement in a simple memory test (P=.021) but not other cognitive measures. Subjects additionally showed improvements on all 5 ABC subscales (P=.001 to 0.027 depending on the scale).29 In a second retrospective trial of 18 patients aged 6 to 19 years, a mean dose of memantine 10.1 mg/d over an average treatment period of 19.3 weeks were “much improved” or “very much improved” on the Clinical Global Impression, with decreases of 6.84 on the ABC-hyperactivity (P=.03) and 9 on the ABC-social withdrawal (P=NS) scales.30 An increase in autistic behaviors, including hyperactivity, lethargy, and irritability was seen in several patients in these studies. The results of studies using galantamine, rivastigmine, and memantine show promise, but should be confirmed in larger RDBPC clinical trials before routine use in treatment of ASD can be recommended.
CONCLUSION
Medications are frequently used to treat ASD-related symptoms, even though most lack evidence to support use and do not carry an FDA indication for their use. Treatment focus in patients with ASD must remain on nonpharmacologic interventions. Medication use should be considered adjunctive only. Pharmacists play a crucial role in reviewing medication use to ensure it is appropriate in this population. This includes application of measuring scales such as the ABC to determine efficacy and assuring that appropriate measures are being followed to minimize or prevent ADRs. Medication use in ASD should be approached as short-term therapy with a plan to closely monitor and discontinue the medication if it is not of benefit to the patient.
REFERENCES
1. Rapin I. The autistic-spectrum disorders. N Engl J Med. 2002;347:302–303.
2. Johnson CP, Myers SM, and the Council on Children with Disabilities. Identification and evaluation of children with autism spectrum disorders. Pediatrics. 2007;120:1183–1215.
3. Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators. Prevalence of autism spectrum disorders-Autism and Developmental Disabilities Monitoring Network, 14 Sites, United States, 2008. MMWR. 2012;61:1–19.
4. Hensley E, Briars L. Closer look at autism and the measles–mumps–rubella vaccine. J Am Pharm Assoc. 2010;50:736–741.
5. Aman MG. Aberrant Behavior Checklist: current identity and future developments. Clin Exp Pharmacol. 2012;2(3). Accessed online at: http://dx.doi.org/10.4172/2161-1459.1000e114 on March 2, 2013.
6. Brinkley J, Nations L, Abramson RK, et al. Factor analysis of the aberrant behavior checklist in individuals with autism spectrum disorders. J Autism Dev Disord. 2007;37:1949–1959.
7. Myers SM, Johnson CP, and the Council on Children with Disabilities. Management of children with autism spectrum disorders. Pediatrics. 2007;120:1162-1182.
8. Coury DI, Anagnostou E, Manning-Courtney P, et al. Use of psychotropic medication in children and adolescents with autism spectrum disorders. Pediatrics. 2012;130:S69–S76.
9. McPheeters MI, Warren Z, Sathe N, et al. A systematic review of medical treatments for children with autism spectrum disorders. Pediatrics. 2011;127:e1312–e1321.
10. Leskovec TJ, Rowles BM, Findling RL. Pharmacological treatment options for autism spectrum disorders in children and adolescents. Harv Rev Psychiatry. 2008;16:97–112.
11. Research Units on Pediatric Psychpharmacology Autism Network. Risperidone in children with autism and serious behavioral problems. N Engl J Med. 2002;347:314–321.
12. Research Units on Pediatric Psychopharmacology Autism Network. Risperidone treatment of autistic disorder: longer-term benefits and blinded discontinuation after 6 months. Am J Psychiatry. 2005;162:1361–1369.
13. Owen R, Sikich L, Marcus RN, et al. Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder. Pediatrics. 2009;124:1533–1540.
14. Marcus RN, Owen R, Kamen L, et al. A placebo-controlled, fixed-dose study of aripiprazole in children and adolescents with irritability associated with autistic disorder. J Am Acad Child Adolesc Psychiatry. 2009;48:1110–1119.
15. Canitano R, Scandurra V. Psychopharmacology in autism: an update. Progr Neuro Psychopharmacol Biol Psychiatry. 2011;35:18–28.
16. Hollander E, Soorya I, Chaplin W, et al. A double-blind placebo-controlled trial of fluoxetine for repetitive behaviors and global severity in adult autism spectrum disorders. Am J Psychiatry. 2012;169:292–299.
17. Davanzo PA, Belin TR, Widawski MH, King BH. Paroxetine treatment of aggression and self-injury in persons with mental retardation. Am J Ment Retard. 1998;102:427–437.
18. McDougle CJ, Brodkin ES, Naylor ST, Carlson DC, Cohen DJ, Price LH. Sertraline in adults with pervasive developmental disorders: a prospective open-label investigation. J Clin Psychopharmacol. 1998;18:62–66.
19. Hollander E, Phillips A, Chaplin W, et al. A placebo controlled crossover trial of liquid fluoxetine on repetitive behaviors in childhood and adolescent autism. Neuropsychopharmacology. 2005; 30:582–589.
20. Mahajan R, Bernal MP, Panzer R, et al. Clinical practice pathways for evaluation and medication choice for attention-deficit/hyperactivity disorder symptoms in autism spectrum disorders. Pediatrics. 2012;130:S125–S138.
21. Research Units on Pediatric Psychopharmacology (RUPP) Autism Network. Randomized, controlled, crossover trial of methylphenidate in pervasive developmental disorders with hyperactivity. Arch Gen Psychiatry. 2005; 2005;62:1266-1274.
22. Jahromi LB, Kasari CL, McCracken JT, et al. Positive effects of methylphenidate on social communication and self-regulation in children with pervasive developmental disorders and hyperactivity. J Autism Dev Disord. 2009;39:395–404.
23. Arnold LE, Aman MG, Cook AM, et al. Atomoxetine for hyperactivity in autism spectrum disorders: placebo-controlled crossover pilot trial. J Am Acad Child Adolesc Psychiatry. 2006;45:1196–1205.
24. Harfterkamp M, van de Loo-Neus G, Minderaa RB, et al. A randomized double-blind study of atomoxetine versus placebo for attention-deficit/hyperactivity disorder symptoms in children with autism spectrum disorder. J Am Acad Child Adolesc Psychiatry. 2012;51:733–741.
25. Chez MG, Aimonovitch M, Buchanan T, Mrazek S, Tremb RJ. Treating autism spectrum disorders in children: utility of the cholinesterase inhibitor rivastigmine tartrate. J Child Neurol. 2004;19:165–169.
26. Handen BL, Johnson CR, McAuliffe-Bellin S, Murray PJ, Harden AY. Safety and efficacy of donepezil in children and adolescents with autism: neuropsychological measures. J Child Adolesc Psychopharmacol. 2011;21:43–50.
27. Hertzman M. Galantamine in the treatment of adult autism: a report of three clinical cases. Int J Psychiatry Med. 2003;33:395–398.
28. Niederhofer H, Staffen W, Mair A. Galantamine may be effective in treating autistic disorder. BMJ. 2002;325:1422.
29. OwleyT, Salt J, Guter S, et al. A prospective, open-label trial of memantine in the treatment of cognitive, behavioral, and memory dysfunction in pervasive developmental disorders. J Child Adolesc Psychopharmacol. 2006;16:517–524.
30. Erickson CA, Posey DJ, Stigler KA, Katschke AR, McDougle CJ. A retrospective study of memantine in children and adolescents with pervasive developmental disorders. Psychopharmacology. 2007;191:141–147.








FDA Issues Complete Response Letter for Pz-Cel to Treat Epidermolysis Bullosa
April 22nd 2024Prademagene zamikeracel is a cell therapy designed to incorporate the functional collagen-producing COL7A1 gene into a patient’s own skin cells. The FDA is asking for additional information on manufacturing practices.

