
- Safety & Recalls
- Regulatory Updates
- Drug Coverage
- COPD
- Cardiovascular
- Obstetrics-Gynecology & Women's Health
- Ophthalmology
- Clinical Pharmacology
- Pediatrics
- Urology
- Pharmacy
- Idiopathic Pulmonary Fibrosis
- Diabetes and Endocrinology
- Allergy, Immunology, and ENT
- Musculoskeletal/Rheumatology
- Respiratory
- Psychiatry and Behavioral Health
- Dermatology
- Oncology
Preferential formulary listing of a proton-pump inhibitor (PPI): Compliance with policy in a Canadian military population
In 2003, the Canadian Forces (CF) drug benefit plan used preferential listing to control costs associated with proton pump inhibitors (PPIs); however, significant expenditures for nonbenefit PPIs continued. A database review was thus conducted to explain this anomalous usage pattern. This study provides further information regarding the effectiveness of preferred listing as a cost-saving measure, noting that adherence to such policies may be less than projected.



Key Points
Abstract
Preferential listing of a single drug is a common strategy for controlling costs within a drug class. In 2003, the Canadian Forces (CF) drug benefit plan used preferential listing to control costs associated with proton pump inhibitors (PPIs). However, significant expenditures for nonbenefit PPIs continued. A database review was thus conducted to explain this anomalous usage pattern. Pharmacy claims for PPIs were reviewed for CF members who received ≥1 PPIs between 2002 and 2005. Documentation entered by pharmacists at the time of prescription processing was also reviewed. A total of 4,738 PPI users were identified, of whom 87% were using the preferred drug. "Failure to respond" was the most common reason for use of nonbenefit PPIs (79.4%), whereas side effects were documented in only 8.3% of such users. This study provides further information regarding the effectiveness of preferred listing as a cost-saving measure, noting that adherence to such policies may be less than projected. Our work also demonstrates the utility of pharmacists' notes for purposes of drug use evaluation. (Formulary. 2008;43:436–444.)
The management of gastropathy has changed dramatically as a result of the development of proton pump inhibitors (PPIs). These agents form an integral part of the treatment plan for various gastric conditions, including peptic ulcer disease, gastroesophageal reflux disease (GERD), Zollinger-Ellison syndrome, and eradication of Helicobacter pylori infection. More recently, PPIs have also been recommended for use in less clearly defined conditions, such as treatment of nonulcer dyspepsia or H pylori eradication among users of nonsteroidal anti-inflammatory drugs (NSAIDs).1–3
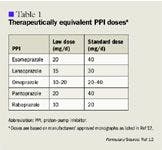
In February 2003, the Canadian Forces (CF) added pantoprazole to the drug benefit list as an unrestricted item; at the same time, all other PPIs were restricted for use in individuals who either did not tolerate or did not respond adequately to a trial of pantoprazole. This agent was selected as the preferred PPI based on clinical evidence, availability of dosage forms, and cost. Little difference in efficacy exists between PPIs when prescribed at equivalent doses (Table 1).5–7 This policy amendment also represented a change in the preferred agent in the drug class (ie, lansoprazole was previously considered as the preferred PPI).
Despite the implementation of this policy change, however, our program has continued to sustain extensive expenditures for nonbenefit PPIs. In fiscal year 2003 to 2004, immediately following the policy change, pantoprazole represented only 50% of costs associated with the PPI class (Can$214,451.98 for pantoprazole vs Can$431,504.52 for all PPIs). As some of this cost represents expenditures for stocking of intravenous (IV) pantoprazole in standardized military medical kits for use during deployments, it can be deduced that a significant portion of CF expenses on PPIs continues to be for nonbenefit items. Further information on the reasons for this anomalous usage pattern could be used to redefine the existing policy, if necessary, and could provide evidence to support similar "rationalization" initiatives for other drug classes.
At the time this study was conducted, our drug benefit program also underwent extensive audit by an external, government-appointed agency.8 We felt that this study was therefore particularly prudent, in that it could not only quantify the true amounts that could be saved through preferential listing, but would also highlight strengths and weaknesses of the existing information on drug usage and expenditures in our healthcare system. This study was therefore conducted primarily to determine the level of conformity with our revised PPI usage policy. Secondary objectives involved description of PPI usage patterns in our population, identification of reasons for use of nonbenefit PPIs, and review of information in our pharmacy claims database.
METHODS


Our original study design also included a separate attempt to validate the reasons for use of a nonbenefit PPI directly with patients by using a structured telephone survey; however, this second phase was to be performed only if the database review indicated that significant noncompliance with our policy (defined as ≥20% of members taking a nonbenefit PPI) was present. This cutoff was determined on the basis of the following projected rates: 5% side effects or product intolerance, 5% nonresponse to the preferred agent, and 10% missing or incomplete information. This survey was not performed, however, because of the results obtained from our database review.
Study population. All Reserve and Regular Forces members of the CF who received ≥1 PPIs between January 1, 2004, and December 31, 2004, were included in the study. Members who received a PPI as part of a combination product for treatment of H pylori infection (ie, the HP-Pac, containing amoxicillin, clarithromycin, and lansoprazole in a fixed combination) were excluded from the review.
Data collection. For each eligible patient, pharmacy records were assessed to obtain the following information: individual identifier, demographic information (sex and age/date of birth), and PPI use (name of PPI[s] prescribed, date of first prescription for PPI[s] prescribed, dosage[s] of PPI[s] prescribed, and, for nonbenefit PPI[s], the reason given for switching from pantoprazole). PPI dose was further categorized in terms of duration (categorized as <2 wk, 2–8 wk, or >8 wk of continuous therapy) and dosage (high- or low-dose, per Table 1).

RESULTS
A total of 4,738 members received a PPI in 2004. As expected in our military population, most members were male (85.2%). The mean age in this cohort (40.2 y; SD=7.99; range, 20–65) was higher than in the general CF population.
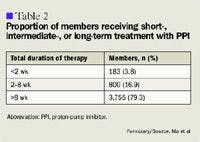
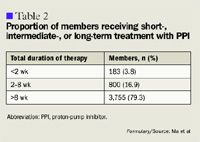
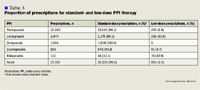
These patients received a total of 27,156 prescriptions for PPIs between January 1, 2002, and January 31, 2005. The mean number of prescriptions per member during this time period was 5.7 (SD=4.8; range, 1–39). Overall, the mean duration of treatment per prescription was 47.3 days (SD=19.5; range, 1–365), although most prescriptions (79.3%) were for courses of >8 weeks' duration (Table 2). The mean duration of treatment did not differ significantly among the 5 different PPIs represented in the database (range, 43.4–50.5 d).

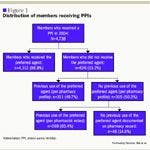
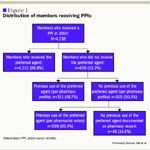
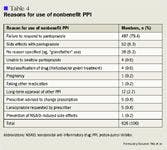
The initial review of the prescription claims records revealed that 86.8% of CF members were receiving the preferred PPI (Figure 1). Of the remaining 626 members receiving a nonbenefit PPI at time of review, prior use of the preferred agent was noted in the members' pharmacy profiles in just under half of the cases (49.7%). However, among those without prior use of pantoprazole documented on their pharmacy claims profile, the pharmacists' notes identified failure to respond to or side effects with the preferred agent in a further 269 members, thus indicating prior use of the preferred agent. Overall, only 39 instances were identified in which no specific rationale was given for use of a nonbenefit PPI. All reasons for use of a nonbenefit PPI are listed in Table 4.
Among patients taking a nonbenefit PPI, the most common reason reported for such use was failure to respond to our chosen PPI (79.4%). However, this group represents only 10% of our overall population of PPI users (497 of 4,738 PPI users). Our review of the records also indicated that, in all instances when "failure to respond" was noted, the dosage of pantoprazole prescribed before initiation of a nonbenefit PPI was ≥40 mg/d.
Among those members currently using a nonbenefit PPI, side effects with the preferred agent (pantoprazole) were reported in the database for 52 individuals. In 15 of these cases, no specific side effects were noted. Among the 37 side effects that were described in greater detail, 25 were gastrointestinal in nature (67.6%; Table 5).
DISCUSSION




This detailed review therefore represents our attempt to quantify the limitations inherent in our drug usage database, which includes documentation from the dispensing pharmacists in addition to information from payor-reimbursed pharmacy claims. Our study illustrates the added value of pharmacists' notes for evaluation of drug usage. At present, most pharmacy-specific software programs do incorporate mechanisms that allow documentation of information related to individual patients' pharmacotherapy, presumably to facilitate ongoing monitoring for drug-related problems, or to identify other patient-specific issues related to medications. Such notes may or may not be standardized, depending on organizational needs and legislative or administrative requirements, but almost all will include functions to document certain "core" types of information, such as side effects or allergic reactions to medications. In our study, the pharmacist notes allowed us to identify a further 5.7% of members whose PPI usage was in accordance with the existing policy, despite pharmacy profiles to the contrary.



Our efforts to quantify the accuracy of our pharmacy claims records is, however, limited. In particular, we did not progress to the survey stage initially proposed as a separate step to validate the accuracy of information in the database. This activity, had it been completed, would have provided us with an opportunity to confirm the rationale for use of a nonbenefit PPI with the patients themselves and could have allowed for identification of other health outcomes associated with specific PPIs. However, one previous study does provide information in this regard, namely to identify that although negative health outcomes (eg, worsening of symptoms and increased frequency of symptoms) did occur among some patients who failed to respond to a new PPI introduced through a formulary change, overall healthcare costs did not increase.13
These study results also indicated similar reasons for use of the nonbenefit PPI as noted in our study, with >70% of patients in whom treatment failed reporting poor symptom control (analogous to our definition of "failure to respond").
As mentioned, a telephone survey was also initially proposed as part of this study, to obtain information regarding patients' willingness to switch to another PPI. Because the absolute number of members receiving a nonbenefit PPI without a prior trial of pantoprazole was low, however, the utility of this segment of the questionnaire is limited. However, previous data from other practice sites have indicated that patients are not averse to trying alternate PPIs or dosage reductions, provided that the risks and benefits of such therapy are adequately described and the option of resuming the previous (effective) treatment is available.14–16 There is no reason to suspect that such attitudes would not prevail in our members as well.
CONCLUSIONS
We employed preferential listing of a single PPI in an attempt to achieve cost savings for our drug benefit plan. However, as demonstrated in our study, full compliance with such therapeutic substitution policies is unlikely to occur. Levels of noncompliance should therefore be anticipated when organizations are projecting the resultant cost savings.
Additional information from pharmacists' notes may be used to confirm compliance when the patient's pharmacy profile indicates discordance with preferential listing policies.
Limitations of the pharmacy profile and databases that are derived from such profiles should be borne in mind when pharmacy records alone are used to conduct drug use evaluations.
At the time this manuscript was prepared, Dr Ma was the Drug Use Evaluation Research Manager, Canadian Forces Health Services, Directorate of Medical Policy, Pharmacy Policies and Standards, Ottawa, Ontario. Mr Gervais is a Drug Use Evaluation Pharmacist, Canadian Forces Health Services, and a clinical pharmacist at the Carling Metabolic Syndrome Clinic, Ottawa, Ontario. Ms Lanouette is the Chief Research Assistant, Canadian Forces Health Services.
Disclosure Information: The authors report no financial disclosures as related to products discussed in this article.
REFERENCES
1. Hunt RH, Fallone C, Veldhuyzen Van Zanten S, et al. Canadian Helicobacter pylori Study Group. Etiology of dyspepsia: Implications for empirical therapy. Can J Gastroenterol. 2002; 16:635–641.
2. McColl K, Murray L, El-Omar E, et al. Symptomatic benefit from eradicating Helicobacter pylori infection in patients with nonulcer dyspepsia. N Engl J Med. 1998;339:1869–1874.
3. Hunt RH, Bazzoli F. Review article: Should NSAID/low-dose aspirin takers be tested routinely for H pylori infection and treated if positive? Implications for primary risk of ulcer and ulcer relapse after initial healing. Aliment Pharmacol Ther. 2004;19(suppl 1):9–16.
4. Amidon PB, Jankovich R, Stoukides CA, Kaul AF. Proton pump inhibitor therapy: Preliminary results of a therapeutic interchange program. Am J Manag Care. 2000;6:593–601.
5. Gerson LB, Hatton BN, Ryono R, et al. Clinical and fiscal impact of lansoprazole intolerance in veterans with gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2000;14:397–406.
6. Dott AG, Johnson L. Rational prescribing: Practice audit and drug switch in dyspepsia management. Int J Clin Pract. 1999;53:599–603.
7. Canadian Agency for Drugs and Technologies in Health. Evidence for PPI use in gastroesophageal reflux disease, dyspepsia and peptic ulcer disease: Scientific report. Optimal Therapy Report-COMPUS MARCH 2007. http://www.cadth.ca/media/compus/reports/compus_Scientific_Report_final.pdf.
8. 2004 NovemberReport of the Auditor General of Canada. Chapter 4: Management of federal drug benefit programs. November 2004. http://www.oag-bvg.gc.ca/internet/English/parl_oag_200411_04_e_14908.html.
9. Yacyshyn BR, Thomson AB. The clinical importance of proton pump inhibitor pharmacokinetics. Digestion. 2002;66:67–78.
10. Holbrook AM; for Ontario GI Therapy Review Panel. OntarioGuidelines for Peptic Ulcer Disease and Gastroesophageal Reflux. Toronto, Ontario: Queen's Printer of Ontario; 2000.
11. The RxFiles Academic Detailing Program. The RxFiles-Drug Comparison Chart Updates, July 2003. Saskatoon, Saskatchewan: Saskatoon Health Region; 2003.
12. Compendium of Pharmaceuticals and Specialties (CPS), 42nd ed. Ottawa, Ontario: Canadian Pharmacists Association/Webcom Ltd; 2007.
13. Raisch DW, Klaurens LM, Hayden C, Malagon I, Pulliam G, Fass R. Impact of a formulary change in proton pump inhibitors on health care costs and patients' symptoms. Dig Dis Sci. 2001;46:1533–1539.
14. Boath EH, Blenkinsopp A. The rise and rise of proton pump inhibitor drugs: Patients' perspectives. Soc Sci Med. 1997;45:1571–1579.
15. Pollock K, Grime J. Strategies for reducing the prescribing of proton pump inhibitors (PPIs): Patient self-regulation of treatment may be an under-exploited resource. Soc Sci Med. 2000;51:1827–1839.
16. Grime J, Pollock K, Blenkinsopp A. Proton pump inhibitors: Perspectives of patients and their GPs. Br J Gen Practice. 2001;51:703–11.

Employers Face Barriers With Adopting Biosimilars
March 1st 2022Despite the promise of savings billions of dollars in the United States, adoption of biosimilars has been slow. A roundtable discussion among employers highlighted some of the barriers, including formulary design and drug pricing and rebates.






