
- Safety & Recalls
- Regulatory Updates
- Drug Coverage
- COPD
- Cardiovascular
- Obstetrics-Gynecology & Women's Health
- Ophthalmology
- Clinical Pharmacology
- Pediatrics
- Urology
- Pharmacy
- Idiopathic Pulmonary Fibrosis
- Diabetes and Endocrinology
- Allergy, Immunology, and ENT
- Musculoskeletal/Rheumatology
- Respiratory
- Psychiatry and Behavioral Health
- Dermatology
- Oncology
A review of nonpharmacologic and pharmacologic therapies for smoking cessation
This article provides information about pharmacologic and nonpharmacologic treatments that are used to help people stop smoking, including the use of varenicline.



Key Points
• Abstract
Cigarette smoking is one of the leading causes of the development of cardiovascular disease and premature death among men and women in the United States. Smoking is associated with increased morbidity and mortality among both smokers and nonsmokers who are exposed to secondhand smoke. Smoking cessation can improve the health and overall outcomes of smokers almost immediately. Multiple attempts at cessation are often necessary to achieve complete abstinence because of the highly addictive properties of nicotine. Many treatment options, both nonpharmacologic and pharmacologic, are available to assist patients who are attempting to quit smoking. Cognitive behavior therapy has been demonstrated to be efficacious, prolonging abstinence rates when used in combination with pharmacologic therapy. Traditional pharmacologic therapies, including nicotine replacement therapy and bupropion, have been demonstrated to be effective in patients who are attempting smoking cessation. The approval of varenicline, the newest agent for smoking cessation, has provided clinicians with an additional treatment option. Clonidine and nortriptyline, although not approved by FDA for smoking cessation, have also been studied in this patient population; results have been conflicting. (Formulary. 2007;43:44–64.)



In addition, cigarette smoke contains several known carcinogens. Of the 4,800 chemicals in cigarette smoke, 69 have been demonstrated to cause cancer.2 Of all cancer deaths, 30% can be attributed to smoking.3 Rates of lung cancer in smokers are significantly greater than in nonsmokers; 87% of all lung cancer deaths are caused by smoking. Male smokers are 23 times more likely to develop lung cancer than nonsmoking men, and female smokers are 13 times more likely to develop lung cancer compared with nonsmoking women.3 Smoking has also been demonstrated to increase the incidence of cancers of the mouth, pharynx, larynx, esophagus, bladder, kidneys, pancreas, cervix, and stomach.3
Smoking is also one of the primary risk factors for the development of chronic obstructive pulmonary disease (COPD), which is associated with significant mortality in smokers.2
Overall, recent statistics demonstrate that male smokers die approximately 13 years earlier than male nonsmokers, and female smokers die approximately 14 years earlier than female nonsmokers.1
Cigarette smoking can also lead to complications with pregnancy. Pregnant women who smoke are more likely to have a preterm or low-birth-weight baby. In the United States, 20% to 30% of low-birth-weight babies and 14% of premature babies are born to women who smoke.2 Learning and developmental disabilities are more prevalent in babies born with low birth weight. Additionally, 10% of all infant deaths in the United States can be attributed to women who smoked during pregnancy.2 Only approximately 30% of women quit smoking when they discover they are pregnant.2 However, in 2004, the percentage of women who smoked during pregnancy was 10.2%, which represents a 42% decrease from 1990.2 US healthcare costs associated with premature infants born to mothers who smoked during pregnancy exceed $350 million each year.2 Additionally, children who are exposed to secondhand smoke from their parents have increased frequencies of colds, ear infections, and asthma exacerbations. As many as 300,000 lower respiratory tract infections in children aged <18 months are caused by the exposure to secondhand smoke in the household.2
Secondhand smoke is almost as detrimental to a person's health as smoking itself.1 The US Environmental Protection Agency (EPA) classifies secondhand smoke from cigarettes as a Group A known carcinogen.2 Approximately 126 million nonsmoking Americans are regularly exposed to secondhand smoke.3 Annually, secondhand smoke is responsible for 3,400 deaths from lung cancer and approximately 46,000 deaths associated with heart disease in nonsmokers.2
PHARMACOLOGY OF NICOTINE
Nicotine was first isolated from the leaves of the tobacco plant Nicotina tab-acum in 1828 and is the main alkaloid found in tobacco. Since its discovery, nicotine has been widely used in a variety of vehicles and may be considered one of the most commonly used drugs of abuse.4
Because of its lipophilic properties, nicotine is readily absorbed through the lungs, buccal membranes, and skin, but its absorption through cell membranes is dependent on a basic pH.5 Cigarette smoke is generally acidic; therefore, the nicotine from cigarettes is not easily absorbed through the buccal route, as the acidity of the smoke changes the pH of the membranes. Smoke from cigars or pipes is of basic pH, allowing for ease of absorption through the buccal route, which consists of an alkalinic environment, and thereby promoting increased blood nicotine levels without inhalation. With cigarettes, inhalation is required for nicotine to be absorbed. A rich blood supply, such as that found in the pulmonary capillaries, is important for absorption; the pulmonary capillary blood flow facilitates absorption of inhaled products through the alveolar capillary interface.5
A cigarette contains 6 to 11 mg of nicotine and delivers approximately 1 mg of nicotine systemically. Bioavailability is variable and can increase as much as 3-fold depending on the puffing technique of the smoker. The half-life of nicotine is approximately 2 hours. Nicotine is extensively metabolized in the liver, but its metabolites are readily eliminated by the kidneys. The rate of elimination is decreased as the pH of the urine rises. Nicotine is also excreted in the breast milk of lactating women.6
The addictive potential of a substance is dependent on the length of time between administration and central nervous system (CNS) reinforcement. Because nicotine reaches the brain approximately 10 to 20 seconds after cigarette inhalation (more rapidly than when nicotine is administered intravenously [IV]), cigarette smoking is especially addictive.5

Nicotine causes an increase in heart rate and blood pressure (BP) through the stimulation of sympathetic ganglia and the adrenal medulla. Nicotine also activates the chemoreceptors of the aortic and carotid bodies, leading to vasoconstriction, tachycardia, and subsequent increases in BP. Nicotine increases the tone and motor activity of the bowel, which can lead to diarrhea, nausea, and vomiting.4,5
Blood levels of nicotine increase over 6 to 8 hours of smoking, with acute tolerance to its effects developing throughout the day. Overnight, with acute abstinence from smoking, nicotine blood levels decrease. This period of cessation and elimination of nicotine from the body allows for resensitization to nicotine's effects. Increases in heart rate are observed in smokers after the first few cigarettes of the day, but no effect on heart rate is observed after several cigarettes are smoked, evidence that acute nicotine tolerance develops.4,5
DRUG INTERACTIONS WITH SMOKING
Cigarette smoking can interfere with the anticipated response or effect of a drug through pharmacokinetic and pharmacodynamic interactions. Many chemicals are present in cigarette smoke that may affect drug disposition. In the past, it was thought that nicotine alone was responsible for alterations in drug kinetic and/or dynamic interactions. It is now known that multiple substances found in cigarette smoke can interact with the hepatic CYP450 system and elicit these changes. Examples of these substances include acetone, pyridine, carbon monoxide, and benzene.8 Classes of compounds known as polycyclic aromatic hydrocarbons (PAHs) are also present in large concentrations in cigarette smoke and are potent inducers of the CYP450 system.8,9 Cigarette smoke is known to selectively induce the activity of CYP1A1, 1A2, and possibly 2E1.8–10 Because of this, smokers are more likely to require higher doses of drugs that are metabolized via these pathways. It should be noted that nicotine replacement therapy (NRT) alone has little, if no, effect on pharmacokinetic drug interactions; rather, PAHs in cigarette smoke are responsible for the majority of these interactions. Pharmacodynamic interactions are more likely to occur with nicotine itself and with NRT.11 There are many drugs of clinical importance that interact with cigarette smoke, including theophylline, tacrine, insulin, propranolol, propoxyphene, benzodiazepines, clozapine/olanzapine, oral contraceptives, tricyclic antidepressants, and inhaled corticosteroids.8,9,12–20
BENEFITS OF CESSATION
Smoking cessation can improve the health and overall outcomes of smokers almost immediately, and the benefits increase as the length of cessation time increases. Twenty minutes after cessation, the heart rate and BP begin to decrease. The carbon monoxide level in a smoker's blood returns to normal 12 hours after the last cigarette smoked. Circulation improves and lung function is increased as soon as 2 weeks after cessation. In 1 to 9 months, former smokers will note a significant decrease in coughing and shortness of breath. At this time, cilia in the lungs regain normal function. The increased risk of CHD is decreased to half that of current smokers at 1 year after smoking cessation. Remaining abstinent from cigarette smoking for 5 years reduces the former smoker's risk of stroke to that of a nonsmoker's; if a former smoker is able to successfully refrain from smoking for 15 years, the risk of CHD is reduced to that of a nonsmoker's.21
Smoking cessation can also lead to financial and social benefits. In July 2007, the average national cost of a pack of cigarettes was $4.34. For those who smoked 1 pack/d, the cost was approximately $30.40/wk and $1,600.00/y.22 As the cost of cigarettes continues to increase, smoking cessation should lead to greater savings. Socially, smoking is not as accepted as it once was. In response to growing evidence of the deleterious effects of secondhand smoke, many states have taken the initiative to pass smoke-free air laws. In a 2006 report by the Surgeon General, it was concluded that there is no level of secondhand smoke that is safe for adult nonsmokers.23 Many hotels and corporations became smoke free in 2006; the enactment of smoke-free workplace regulations is ongoing.23 Many establishments such as restaurants, bars, and entertainment venues have also become smoke free.
OBSTACLES TO CESSATION
According to recent data from the American Cancer Society (ACS), >70% of current smokers in the United States report that they want to quit smoking. However only 5% to 10% of those are able to do so in any given attempt. Those attempting to quit smoking may encounter several obstacles that derail the cessation attempt.3
One of the most common concerns smokers have regarding cessation is weight gain. During cessation, the stimulant effect of nicotine is no longer experienced, and many may turn to food as a substitute for the pleasurable effects experienced with smoking. The average weight gain that occurs in former smokers is <10 pounds.21 To help with this obstacle to cessation, healthcare professionals should counsel patients to begin walking as a way to reduce weight gain and to decrease stress.
Cigarette smoking is also a habitual activity. Smokers may associate the act of smoking with certain daily activities such as drinking coffee, completion of a meal, or driving. These activities may trigger urges to smoke while patients are attempting to quit. Patients should identify their personal triggers and develop alternative behaviors (eg, chewing gum while driving, going for a walk after meals).
Those attempting to quit may also find it more difficult if they live with or socialize with smokers. An integral part of smoking cessation is a strong support system. Smokers contemplating quitting should discuss their intentions with family members and friends.
Because of these obstacles and the addictive nature of nicotine, smoking cessation is very difficult for many smokers; often, several attempts are needed to achieve complete cessation. There are multiple treatment options, both nonpharmacologic and pharmacologic, to aid patients attempting smoking cessation.
NONPHARMACOLOGIC THERAPIES
Cognitive behavioral therapy. Clinicians have screening and intervention modalities that can be used to promote smoking cessation. Both the Agency for Health Care Policy and Research (AHCPR) and the American Psychiatric Association (APA) have set forth similar guidelines to help clinicians target this risk factor in their patients.24–26 All smokers should be asked if they are willing to commit to cessation and if patients are agreeable, the clinician should discuss the various treatment options available.
Both group and individual counseling sessions are effective strategies for smoking cessation; many trials that evaluate the effectiveness of pharmacologic therapy also use cognitive behavioral therapy as an adjunct. Group counseling sessions may include group meetings, lectures, development of coping strategies, and provision of information to prevent relapse. The importance of cessation and continued abstinence should be addressed at each encounter. Obstacles such as weight gain, withdrawal symptoms, changes in mood, and lack of support system and various coping strategies should also be discussed. Treatment should include strategies that help the patient identify triggers for smoking and employ effective techniques that decrease the likelihood of relapse. Also of great importance is support between sessions. Although short counseling encounters may be sufficient for some patients, more concentrated therapy may be warranted for others. Programs that allow for direct personal communication tend to improve the chances of successful smoking cessation.24 This was demonstrated by the results of a randomized trial that assessed a smoking cessation help line in California.27 Patients were randomized to either a treatment group, in which they received as many as 7 counseling sessions, or to a control group, in which patients could receive counseling only if they called the help line after randomization. All patients enrolled received self-help materials. More counseling was provided to those in the treatment group than to those in the control group (72.1% vs 31.6%). Those randomly assigned to the treatment group had higher cessation rates at 1, 3, 6, and 12 months compared with patients in the control group (P<.001).
Hypnotherapy. Some patients have used hypnotherapy as an aid for smoking cessation, especially in attempting to alleviate or lessen the urge to smoke. A meta-analysis of 9 randomized trials of hypnotherapy for smoking cessation was conducted; comparative interventions included hypnotherapy with or without counseling, hypnotherapy with or without group therapy, psychological treatments, and no therapy.28 The authors concluded that hypnotherapy did not demonstrate greater rates of cessation at 6 months compared with other interventions or with no therapy.
Acupuncture. Many smokers have used acupuncture in an attempt to limit or alleviate nicotine withdrawal symptoms. One study examined the effects of acupuncture on smoking cessation in 46 patients who were followed for 5 years.28 Enrolled patients had smoked for an average of 23 years, typically smoked 10 to 30 cigarettes/d, agreed not to use any other form of cessation modalities during the 3-week treatment phase, and were willing to quit smoking. A total of 26 patients received acupuncture in specific areas that are thought to correspond to areas of the body affected by smoking, such as the lungs and mouth. The control group consisted of 20 patients who received acupuncture in areas that are not thought to correspond to areas affected by smoking. Patients received treatment twice weekly for 3 weeks. Patients were asked how many cigarettes they smoked, and blood samples were drawn to determine concentrations of cotinine and thiocyanate; this enabled researchers to determine whether patients had smoked in the preceding few weeks. At the 5-year follow-up, 4 patients from the acupuncture group had maintained abstinence compared with 2 patients from the control group. Although this study was limited by its small sample size, further studies are warranted to confirm the results observed.
A meta-analysis of 22 randomized studies was conducted to determine the effect that acupuncture and other related therapies (acupressure, laser therapy, and electrostimulation) have on smoking cessation versus placebo or no therapy.30 The authors concluded that these studies did not clearly demonstrate a benefit with these alternative methods for smoking cessation.30 The use of these methods may be considered for patients in whom other smoking cessation therapies have failed.
PHARMACOLOGIC THERAPIES
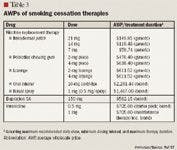
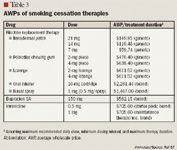
Nicotine replacement therapy. Typically, the first-line agents for smoking cessation are NRTs unless these agents are contraindicated. NRT is readily available to patients; most dosage forms are accessible over-the-counter (OTC). Dosage forms include a transdermal patch, chewing gum, lozenge, oral inhaler, and nasal spray. A prescription is required for the nicotine inhaler and nasal spray; all other forms are available without a prescription.
NRT was the first smoking cessation aid approved by FDA. As previously mentioned, nicotine is the primary addictive chemical found in cigarette smoke and results in reinforcing effects when it reaches the CNS.5 During abrupt smoking cessation, blood levels of nicotine decline rapidly, leading to withdrawal symptoms. NRT was developed to mimic the effects of inhaled nicotine on the body and to replete the blood levels of nicotine that are lost during smoking cessation, thereby helping to alleviate withdrawal symptoms and to prevent smoking relapse.
The transdermal nicotine patch delivers a continuous level of nicotine into the bloodstream while worn (for ≤24 h), making the patch an effective and convenient delivery system.31 However, the patch has minimal effects on acute cravings. The patch is available in 3 strengths (7, 14, and 21 mg/d) and is designed to be used as step-down therapy. The starting dose is dependent on the number of cigarettes/d that patients usually smoke. Patients who smoke ≥10 cigarettes/d should initiate therapy with the 21-mg/d patch; those smoking <10 cigarettes/d should begin therapy with the 14-mg/d patch. When therapy is initiated with the 21-mg/d patch, this dosage should be continued for 6 to 8 weeks before patients step down to the 14-mg/d patch. This new dosage should be continued for an additional 2 to 4 weeks before patients step down to the 7-mg/d patch. This last dosage should be continued for an additional 2 to 4 weeks. If therapy is initiated with the 14-mg/d patch, a similar step-down schedule is followed. Early morning cravings can be reduced when the patch is worn overnight.31 If patients are unable to tolerate wearing the patch for the full 24 hours because of sleep disturbances, the patch may be removed at bedtime; a new patch should be used in the morning.

Nicotine polacrilex gum and lozenges are available in various strengths and flavors.32,33 These dosage forms are especially beneficial for those patients who experience cravings throughout the day; nicotine is only released when the gum or lozenge is used, thus simulating the act of smoking and alleviating a craving. The dosage of the gum or lozenge is based on the number of cigarettes/d that patients usually smoke. Individuals who smoke ≥25 cigarettes/d should use the 4-mg dose of nicotine gum; individuals who smoke <25 cigarettes/d should use the 2-mg dose of nicotine gum. The nicotine lozenge is dosed based on the usual time to first cigarette. Individuals who usually smoke their first cigarette within 30 minutes of awakening should use the 4-mg dose of nicotine lozenge, whereas those who do not smoke for ≥30 minutes after awakening should use the 2-mg dose of nicotine lozenge. Therapy with either the gum or the lozenge should continue for 12 weeks. Both dosage forms follow a similar dosing interval taper: doses should be administered every 1 to 2 hours for the first 6 weeks, every 2 to 4 hours for the next 3 weeks, and every 4 to 8 hours for the final 2 weeks.32,33
The effectiveness of the gum or lozenge is highly dependent on proper administration technique to ensure adequate drug delivery. Patients should be counseled on proper chewing technique before they use nicotine gum. Patients should be instructed to begin chewing until they experience a tingling or a pepper-like taste. This sensation is indicative of nicotine release. Once this is noted, patients should then place the gum between the cheek and gum line. The gum should remain there until the tingling feeling or pepper-like taste subsides, and then the entire process should be repeated. This cycle should be continued until patients no longer experience tingling or the pepper-like taste; at that point, the gum can be discarded. This entire process takes approximately 30 minutes and should be repeated for each piece of gum administered. If patients continue to have cravings after the administration of 1 piece, another piece can be used immediately thereafter; however, 2 pieces should not be administered concomitantly. The maximum dosage is 24 pieces/d.32 Nicotine gum should also not be used within 15 minutes of eating or drinking, as this can diminish absorption through the buccal cavity.
The nicotine lozenge should be allowed to completely dissolve in the mouth; it should not be chewed, bitten, or swallowed. Patients will experience a tingling or warm sensation while the lozenge is melting, evidence that nicotine is being released. The lozenge should occasionally be moved around in the mouth while it is melting. It will take approximately 20 to 30 minutes for a lozenge to completely dissolve. The maximum dosage is 20 lozenges/d.33 Patients should not use a lozenge within 15 minutes of eating or drinking and should refrain from eating and drinking during lozenge administration.
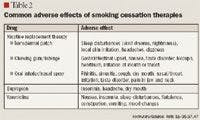
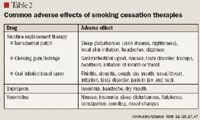
The most common adverse events associated with the nicotine gum and lozenge include gastrointestinal upset, nausea, taste disorder, hiccups, heartburn, and irritation of mouth or throat (Table 2).32,33
The nicotine inhaler and nasal spray deliver nicotine to the bloodstream more rapidly than the patch does, at a rate similar to that observed with the gum and lozenge.31–35 The nicotine inhaler is puffed like a cigar, as the nicotine is absorbed via the buccal cavity. This is unlike smoking a cigarette, in which nicotine is absorbed through the pulmonary capillaries during inhalation. The nicotine inhaler is available in 1 strength, a 10-mg cartridge that delivers 4 mg of nicotine. This dosage form should be used in patients who smoke <20 cigarettes/d only. The inhaler should be puffed continuously for 20 minutes; each cartridge will last for approximately 20 minutes when it is used properly.34 Ten puffs of the inhaler is equivalent to 1 puff of a cigarette. The length of treatment varies from 3 to 6 months. During the first 12 weeks, patients use 6 to 16 cartridges/d; the dosage is gradually tapered to 6 to 12 cartridges/d over the next 12 weeks. Therapy should be tailored to each individual, as there is no defined tapering schedule available.34 The maximum dose is 16 cartridges/d. If abstinence is not achieved by Week 4, therapy with the inhaler should be discontinued. Patients should then re-evaluate smoking cessation motives and, when appropriate, attempt smoking cessation again.
The most common adverse events associated with use of the nicotine inhaler include local irritation of the mouth and throat, cough, rhinitis, taste disorder, pain in jaw and neck, tooth disorders, and sinusitis (Table 2).34
The nicotine nasal spray has the most rapid onset of action compared with the other dosage forms.31–35 The nasal spray is available in only 1 strength, 0.5 mg/ spray (1 mg/dose). Each dose consists of 1 spray per nostril. Patients should be counseled not to sniff, swallow, or inhale through the nose during administration, and the head should be tilted slightly back to optimize delivery. Treatment duration is approximately 14 weeks, with a maximum recommended duration of 6 months. The first 8 weeks of therapy should consist of administration of 1 to 2 doses/h, with a minimum of 8 doses/d.35 As with the inhaler, there is no predefined tapering schedule, but ideally, dosages should be decreased over the next 5 weeks. This can be done by decreasing the dose to 1 spray/administration or by extending the interval between doses. The maximum recommended dose is 5 doses/h or 40 doses/d.
Side effects such as local (nasal and/or ocular) irritation should be taken into consideration, as these may decrease adherence and efficacy. Other common adverse effects associated with the nicotine nasal spray include rhinitis, throat irritation, cough, sneezing, and watery eyes (Table 2).35
Hajek et al36 conducted a randomized, controlled study at 2 sites to compare the efficacy among various NRTs (gum, transdermal patch, inhaler, and nasal spray). Patients were included in the study if they were aged ≥18 years, smoked ≥10 cigarettes/d, expressed a desire to quit, were in overall good health, had not attempted cessation with NRT in the preceding 3 months, were not receiving treatment for a psychiatric disorder, and did not have a contraindication to NRT. A total of 504 patients were included in the study; there were no statistically significant differences among patients in regard to baseline characteristics. Patients were randomized to receive nicotine gum (n=127), transdermal patch (n=124), nasal spray (n=126), or inhaler (n=127). The study duration was 12 weeks, and patients were evaluated during clinic visits at their quit date and at Weeks 1, 4, and 12.
Continued abstinence rates at Week 12 were 19.7% for the gum, 21.0% for the patch, and 23.8% for both the nasal spray and the inhaler. These abstinence rates were confirmed by measurements of saliva cotinine levels and expired carbon monoxide levels of <10 parts per million (ppm). Patients randomized to the transdermal patch demonstrated the highest level of treatment adherence, and this dose form was also deemed the easiest to use during the first week of the study. Patients randomized to the nasal spray had the lowest saliva cotinine levels. Although the nasal spray has the fastest onset of action, this dose form was associated with a higher incidence of adverse effects such as nasal irritation and was underused. Many patients noted embarrassment as their reason for discontinuing therapy with the nicotine inhaler. At study end, the various formulations studied did not differ significantly with respect to overall abstinence rates, withdrawal symptoms, cravings, or weight gain.36
Several issues must be taken into consideration when healthcare professionals and patients are choosing an NRT dosage form. As previously mentioned, the nicotine patch has been associated with vivid dreams and therefore should be used cautiously in patients with a significant psychiatric history (eg, history of post-traumatic stress disorder, schizophrenia, and bipolar disorder). In light of the technique required for proper drug delivery, patients with poor dentition or cognitive defects should refrain from the use of nicotine gum. Patients should be counseled not to smoke while they are wearing the nicotine patch, as this dose form releases nicotine continuously. Nicotine has been demonstrated to acutely raise BP and heart rate; this is also true for NRT. Because of this, NRT should be used cautiously in patients with a history of cardiovascular disease and should be avoided in patients with uncontrolled hypertension, a recent history of myocardial infarction (MI) (within approximately 1 mo before the initiation of NRT), serious arrhythmias, or unstable angina unless clinically indicated.55–59 The most common adverse events associated with the various dose forms of NRT are summarized in Table 2.31–35,37,47
Bupropion. FDA approved bupropion sustained-release tablets in 1997 as an aid for smoking cessation. Bupropion is an antidepressant with a structure chemically unique from that of mono-amine oxidase inhibitors (MAOIs), tricyclic antidepressants, and selective serotonin reuptake inhibitors (SSRIs). Bupropion's exact mechanism of action as an antidepressant and as a smoking cessation agent is not fully understood. It is thought that bupropion's actions are mediated by mechanisms involving the dopaminergic and noradrenergic systems.37
Bupropion sustained-release tablets are approved for smoking cessation at a dose of 150 mg once daily for 3 days; the dose should then be titrated to 150 mg twice daily. Treatment should be initiated 1 week before the set quit date and should then be continued for approximately 7 to 12 weeks.37 Preliminary response can be observed after 1 to 2 weeks of therapy.37 In patients with severe hepatic cirrhosis, bupropion should be prescribed with caution because of the accumulation of active metabolites. In these patients, bupropion should be dosed at ≤150 mg every other day. Dosage or frequency reductions for mild-to-moderate hepatic cirrhosis or renal impairment may be warranted; however, no specific guidelines are currently available.37
Adverse events associated with bupropion therapy are generally mild and may include insomnia, headache, and dry mouth (Table 2).37 Administration of the second dose of bupropion earlier in the day (but ≥8 h after the first dose) may minimize the incidence of insomnia. An increased risk of seizures is a less common but serious adverse effect that has been associated with bupropion therapy; bupropion is therefore contraindicated in patients with a history of a seizure disorder, bulimia, or anorexia.37,39 Bupropion should also be avoided in cases of recent or previous head trauma, severe cirrhosis, CNS tumor, and use of medications that may lower the seizure threshold.37 This increased risk of seizures tends to be dose dependent.39
Bupropion is also indicated for the treatment of depression, and as with all FDA-approved antidepressants, this agent's labeling includes a warning regarding a potential increase in the incidence of suicidal behaviors in children, adolescents, and young adults aged ≤24 years. This increased risk is typically observed during the first few months of therapy. Patients treated with bupropion should therefore be closely monitored when therapy is initiated or dosages are titrated.37
The efficacy of sustained-release bupropion versus placebo was evaluated over 52 weeks in a double-blind, randomized, placebo-controlled trial.38 Patients were included for participation in the study if they were aged ≥18 years, had smoked ≥15 cigarettes/d for the past year, expressed a desire to stop smoking, and were in overall good health. No statistically significant differences were noted among randomized patients (N=615) in regard to baseline characteristics. Patients were randomized to receive bupropion 100, 150, or 300 mg/d (given in 2 divided doses) or placebo for 7 weeks. Patients began therapy 1 week before the anticipated quit date. Counseling was provided at study initiation, weekly during the treatment phase, and at Weeks 8, 12, 26, and 52. Self-reported discontinuation was confirmed by carbon monoxide concentration measurements of <10 ppm in expired air.
At the conclusion of the treatment phase, rates of smoking cessation were 28.8%, 38.6%, 44.2%, and 19.0% among patients treated with bupropion 100, 150, and 300 mg/d or placebo, respectively (P<.001). After 1 year, smoking cessation rates were 19.6%, 22.9%, 23.1%, and 12.4%, respectively. The cessation rates at 52 weeks for the bupropion 150-mg/d group (P=0.02) and the 300-mg/d group (P=.01) were significantly higher compared with the rates observed with placebo. The cessation rate for the 100-mg/d group at 1 year was not significantly higher than the cessation rate observed with placebo (P=.09). Rates of adverse events that necessitated early treatment termination were comparable among groups. Less weight gain was noted among patients treated with higher dosages of bupropion (weight gain, 100 mg/d: 2.3 kg; 150 mg/d: 2.3 kg; 300 mg/d, 1.5 kg; placebo, 2.9 kg).38
Hays et al40 examined the efficacy of sustained-release bupropion in the prevention of smoking relapse following cessation with pharmacologic intervention. Patients were included for participation if they were aged ≥18 years, had smoked ≥15 cigarettes/d for the past year, expressed a desire to stop smoking, and were in overall good health. Self-reported abstinence was confirmed by carbon monoxide concentration measurements of <10 ppm in expired air. A total of 784 patients received open-label sustained-release bupropion 150 mg/d for 3 days followed by 300 mg/d administered in 2 divided doses for 7 weeks. Patients who abstained from smoking throughout the 7-week treatment phase were then randomized to either continued bupropion therapy or to placebo for an additional 45 weeks of treatment (52 weeks of treatment in total). At the completion of the treatment phase, patients were followed for an additional year to determine cessation rates.
The point prevalence of smoking abstinence was greater in the bupropion group compared with the placebo group at the completion of Week 52 (55.1% vs 42.3%; P=.008). The rate of smoking cessation was also greater in the bupropion group than in the placebo group at Week 78 (47.7% vs 37.7%; P=.034); however, no significant differences were noted between the 2 groups at the final follow-up (Week 104). Patients in the bupropion group had experienced less weight gain than those in the placebo group at Weeks 52 and 104 (3.8 kg vs 5.6 kg; P=.002 and 4.1 kg vs 5.4 kg; P=.016, respectively). The authors concluded that patients who remained abstinent after 7 weeks and then continued bupropion therapy had delayed relapse rates and less weight gain compared with patients who were randomized to placebo.40
Jorenby et al41 conducted a double-blind, placebo-controlled study to compare the efficacy of the nicotine transdermal patch, bupropion alone, a bupropion/patch combination, and placebo for smoking cessation. Patients were included for participation if they were aged ≥18 years, had smoked ≥15 cigarettes/d for the past year, were motivated to quit, and weighed ≥45.4 kg. There were no statistically significant differences in baseline characteristics among the study groups. Of the patients screened, 893 met the inclusion criteria; 244 received sustained-release bupropion, 244 received the patch, 245 received the bupropion/patch combination, and 160 received placebo. Treatment groups consisted of sustained-release bupropion for 9 weeks (150 mg/d for 3 days followed by 300 mg/d given in 2 divided doses) or placebo in addition to 8 weeks of therapy with the patch (21 mg/d for Weeks 2 through 7, 14 mg/d for Week 8, and 7 mg/d for Week 9) or placebo. The intended quit day was generally Day 8. The primary outcome measure was the rate of abstinence at 6 and 12 months of follow-up. This primary outcome measure was confirmed by the measurement of carbon monoxide concentration ≤10 ppm in expired air. Secondary outcomes included withdrawal symptoms, weight gain, and changes in Beck Depression Inventory scores.
The continued cessation rates at 12 months were highest for patients who received the bupropion/patch combination compared with the other groups (bupropion, 30.3%; patch,16.4%; bupropion/patch combination, 35.5%; placebo, 15.6%). Weight gain was significantly lower in the bupropion/patch group than in all other treatment groups (bupropion, 1.7 kg; patch, 1.6 kg; bupropion/patch combination, 1.1 kg; placebo, 2.1 kg; P<.05).41 It should be noted that the tapering schedule for the patch in this study differed from that recommended by the manufacturer.
Varenicline. Varenicline was approved on May 10, 2006, as an aid to smoking cessation therapy. This drug is the only approved non-nicotine agent that was developed specifically for smoking cessation.42 Development of varenicline was based in part on the effects of cytisine, a partial agonist of the alpha4-beta2 nicotinic acetylcholine receptors; cytisine is used in Europe for smoking cessation.43,44 Varenicline, also a partial agonist of the alpha4-beta2 subunit of the nicotinic acetylcholine receptor, was designed using the chemical structure of cytisine as a base and was modified to have a higher affinity for the alpha4-beta2 receptors, a structure that was hoped would increase potency and improve efficacy.45
Varenicline exhibits a dual mechanism of action. It binds with high affinity and selectivity to the alpha4-beta2 nicotinic acetylcholine receptors and stimulates receptor-mediated activity. It does so at significantly lower levels than nicotine, and in vitro studies have demonstrated that varenicline produces 68% of the response observed with nicotine binding to these receptors.42,45–47 Varenicline also acts as an antagonist by competitively inhibiting the ability of nicotine to bind to the alpha4-beta2 receptors and thus stimulate the mesolimbic dopamine system. In vivo studies have demonstrated that varenicline inhibits nicotine stimulation of the mesolimbic dopamine system by 66% and produces 32% to 60% of the response observed with nicotine.45 Varenicline therefore alleviates nicotine withdrawal symptoms and cravings without causing dependency, while also blocking the reinforcing effects of repeated nicotine use.
Steady-state levels of varenicline are reached within 4 days of repeated administration.47 This limits the drug's use in acute nicotine withdrawal situations (eg, hospitalized patients). Absorption is virtually complete after oral administration, and bioavailability is not affected by food or administration time. Unlike nicotine, varenicline is not metabolized hepatically, and this agent is primarily excreted unchanged in urine.47 Mild-to-moderate renal impairment does not warrant dosing adjustment. Severe renal insufficiency and end-stage renal disease have been demonstrated to increase the area under the curve (AUC) by 2- to 3-fold; therefore, dosing adjustments are necessary in this patient population.47
The most common adverse effect associated with varenicline use is nausea (Table 2).47 Varenicline has moderate affinity for the serotonin 5-HT3 receptor, which may explain this adverse effect. In studies, mild-to-moderate nausea was reported by approximately 30% of patients receiving varenicline 1 mg twice daily and 16% of patients receiving varenicline 0.5 mg twice daily.46–48 The nausea was usually transient, with a median duration of 12 to 20 days.46,49 Only approximately 3% of patients discontinued treatment with varenicline because of nausea.46,48,50 Efficacy and safety studies have demonstrated that the incidence of nausea is significantly reduced when varenicline doses are titrated over 1 week.47 If nausea persists, a dose decrease should be considered. Insomnia, sleep disturbances, flatulence, constipation, and vomiting were also observed in >5% of study patients (Table 2).47
Doses should be titrated over 1 week, with an initial dose of 0.5 mg once daily for Days 1 to 3, then 0.5 mg twice daily for Days 4 to 7, then 1 mg twice daily (the recommended dose) thereafter. The maximum dose for patients with severe renal impairment is 0.5 mg twice daily. Patients should be counseled to take varenicline after meals and with a full glass of water. Patients should begin therapy 1 week before the set quit date and continue treatment for 12 weeks.47 After 12 weeks, those patients who have successfully stopped smoking should continue therapy for an additional 12 weeks, as this has been demonstrated to significantly improve the rates of continued abstinence. This benefit has been demonstrated to extend to 52 weeks after initiation of therapy.47 Patients who have not succeeded in smoking cessation during the first 12 weeks should not continue with an additional 12-week course but should be encouraged to again attempt cessation once ready.
There are currently no contraindications identified for varenicline therapy.47 Varenicline has been studied in combination with digoxin, warfarin, bupropion, cimetidine, metformin, and the transdermal nicotine patch. No clinically significant pharmacokinetic drug interactions have been noted. Although varenicline has not been demonstrated to affect the pharmacokinetics of bupropion, the safety of the combination has not been studied. The incidence of nausea, headache, vomiting, and dizziness is greater when varenicline is used in combination with NRT, although this combination has no effect on nicotine pharmacokinetics.47
A recent postmarketing case report has suggested the possibility of an interaction between varenicline and immediate-release amphetamine-dextroamphetamine.51 An 18-year-old man who had a 3-year smoking history attempted smoking cessation using varenicline. The patient was already taking immediate-release amphetamine-dextroamphetamine 30 mg twice daily on days he worked for the treatment of attention-deficit/hyperactivity disorder (ADHD). The patient was up-titrated to varenicline 1 mg twice daily as recommended by the manufacturer. After a 23-day lapse in compliance with amphetamine-dextroamphetamine treatment, the patient resumed therapy at the prescribed dose of 30 mg twice daily. Smoking cessation was maintained from Days 8 to 25 of varenicline therapy. He began smoking again on Day 25, 48 hours after resuming amphetamine/ dextroamphetamine therapy. Amphetamines are effective in ADHD because of their ability to increase dopamine levels in the brain. It is hypothesized that by increasing dopamine concentration in the mesolimbic system, amphetamine-dextroamphetamine may produce activity similar to that of nicotine. It has also been suggested that large doses of amphetamines may competitively inhibit varenicline binding to alpha4-beta2 receptors. Because of the strict exclusion criteria of the published efficacy trials, interactions between varenicline and other drugs may not be noted until postmarketing case reports like this one are published.
Several postmarketing reports of suicidal thoughts and aggressive or erratic behavior in patients taking varenicline have recently been reported to FDA.52 Pfizer, the manufacturer of varenicline, has submitted several case reports of suicidal ideations to FDA for review. Early assessments have suggested that many of the cases of depressed mood and suicidal ideations are new in onset and occur days to weeks after initiation of varenicline therapy.52 However, the relationship between the drug and these complaints is not clear. Nicotine withdrawal alone has been known to exacerbate underlying psychiatric diseases, although some patients with these suicidal thoughts or aggressive or erratic behavior did not have known psychiatric conditions, and not all had yet successfully quit smoking. One case has been reported of a varenicline-treated patient exhibiting erratic and aggressive behavior that ultimately led to the patient's death.52 In this case, the patient had also consumed alcoholic beverages on the night of the behavior changes. The potential interaction between varenicline and alcohol is being investigated. FDA is currently reviewing further cases and information provided by Pfizer and will communicate the results of its analysis with the public when complete. In the meantime, FDA recommends that patients taking varenicline should be monitored for any behavior and mood changes. The agency also recommends that patients should be encouraged to contact their healthcare providers should they experience any changes in mood or behavior and also to use caution when driving or operating machinery until they know how varenicline will affect them.52
In January 2008, Pfizer updated the labeling for varenicline to include a warning about serious neuropsychiatric symptoms associated with therapy. Similar to FDA recommendations, the updated labeling recommends that patients should be monitored for changes in behavior, agitation, depressed mood, and suicidal ideation or behavior. The labeling also notes that the safety and efficacy of varenicline have not been established in patients with psychiatric illnesses such as schizophrenia, bipolar disorder, and major depressive disorder, as these patients were not included in premarketing studies of varenicline.47
Varenicline has been demonstrated to be effective as an aid for smoking cessation in several clinical trials.46,48,50 Greater efficacy was demonstrated with varenicline versus placebo in a 7-week trial in which bupropion was included as an active control.46 Male and female smokers aged 18 to 65 years who had smoked an average of 10 cigarettes/d during the previous year without cessation for a period of >3 months and who were considered to be in good health were included in the trial. Participants (N=638) were randomized to receive varenicline 0.3 or 1 mg once daily, varenicline 1 mg twice daily, sustained-release bupropion 150 mg twice daily (titrated from 150 mg daily for 3 d), or placebo. Efficacy was measured primarily by the continuous quit rate (CQR), which was confirmed by carbon monoxide measurements #10 ppm, for any 4 weeks (ie, complete abstinence for any 28-d period during the treatment phase of the trial). Secondary efficacy measures included the confirmed CQRs (confirmed by carbon monoxide measurements) for Weeks 4 through 7 and the CQRs from Week 4 through Weeks 12, 24, and 52.46
A total of 48% of participants in the varenicline 1-mg twice daily group successfully abstained from smoking for 4 weeks compared with 17% of patients in the placebo group (P<.001). A total of 33% of patients in the bupropion group had CQR for 4 weeks, significantly higher than in placebo group (P=.002). CQRs confirmed by carbon monoxide measurements for Weeks 4 to 7 were also significantly higher among all varenicline dose groups compared with placebo (varenicline 0.3 mg once daily vs placebo, P<.05; varenicline 1 mg once daily vs placebo, P≤.01; varenicline 2 mg twice daily vs placebo, P≤.001). Response rates among patients treated with varenicline 1 mg twice daily were 3 times greater than rates in patients treated with placebo (40.8% vs 13.8%; P≤.001). The long-term quit rates at 52 weeks were also significantly higher among patients treated with varenicline 1 mg twice daily compared with those treated with placebo (14.4% vs 4.9%; P≤.01). Although this trial suggested the superiority of varenicline over bupropion, it was not designed to detect statistical significance between the treatments.46
Two identically designed trials were carried out at different sites to compare the efficacy of varenicline with that of bupropion and placebo.48,50 Both trials were double-blind, placebo-controlled, multicenter studies that consisted of a 12-week treatment period with follow-up until Week 52. Patients aged 18 to 75 years who had smoked ≥10 cigarettes/d during the past year, had maintained abstinence for <3 months within the past year, and who were motivated to quit smoking were eligible for enrollment in the studies. Participants (N=2,052) were randomized to receive varenicline, sustained-release bupropion, or placebo for 12 weeks. Active drugs were titrated to full doses over 1 week. Varenicline was initiated at 0.5 mg daily for Days 1 to 3 and then increased to 0.5 mg twice daily for Days 4 to 7. Doses were then increased to 1 mg twice daily; this dose was maintained until the end of the active treatment period. Bupropion was initiated at 150 mg daily for Days 1 to 3 and then increased to 150 mg twice daily thereafter. All interventions were initiated 1 week before the set quit date. During the 12-week treatment phase, participants attended brief individual counseling sessions weekly for relapse prevention. Patients who completed the 12 weeks of treatment entered the nontreatment follow-up phase from Weeks 13 to 52.48,50 The primary outcome measure was the 4-week CQR confirmed by exhaled carbon monoxide measurements ≤10 ppm for Weeks 9 to 12. Secondary end points included continuous cessation periods for Weeks 9 through 24 and for Weeks 9 through 52.
In both studies, varenicline was demonstrated to be superior to bupropion for CQRs for Weeks 9 to 12; varenicline's superiority was also demonstrated for continuous cessation for Weeks 9 through 24. A total of 44% of varenicline-treated participants maintained continuous abstinence during Weeks 9 to 12 compared with 29.5% of bupropion-treated patients (P<.001) in 1 trial, and 43.9% of varenicline-treated patients met this end point compared with 29.8% of bupropion-treated patients (P<.001) in the other trial. Superiority of varenicline to sustained-release bupropion for continuous cessation during Weeks 9 to 52 was demonstrated in only 1 of the trials (first trial, 23% vs 14.6%; P=.004; second trial, 22% vs 16.1%; P=.057).48,50 Mild nausea was the most common adverse effect observed among varenicline-treated patients in both trials. Insomnia was the most common adverse event observed among bupropion-treated patients.48,50
Although the superiority of varenicline over bupropion was demonstrated in these trials, one limitation of the study design should be noted. Participants who had any previous exposure to bupropion, whether it was for smoking cessation or depression, were excluded. This was to ensure a clear comparison between the 2 drugs. However, this design limits the generalization of the results to the majority of patients seeking aid in smoking cessation. One therapy often fails in patients, who then may try the therapy again or try a different therapy. There have been no clinical trials to date that have examined the efficacy of varenicline in patients who have not achieved smoking cessation with sustained-release bupropion. Therefore, efficacy in these patients cannot be predicted.
Other pharmacologic therapies. Clonidine and nortriptyline are sometimes used off-label for aid in smoking cessation. A meta-analysis was conducted to evaluate the use of clonidine versus placebo for smoking cessation; most studies included in this analysis did not demonstrate significant efficacy with clonidine.53 Adverse effects associated with clonidine treatment (including drowsiness, fatigue, dry mouth, dizziness, hypotension, and constipation) also limit its use for smoking cessation.51 Similarly, nortriptyline was not demonstrated to significantly decrease withdrawal symptoms when this agent was studied in combination with the nicotine patch.54 Another study evaluated the effectiveness of nortriptyline alone versus placebo for smoking cessation. Patients randomized to the nortriptyline group of this double-blind, prospective study had higher cessation rates compared with those who received placebo (55.9% vs 23.3%; P<.001). Anticholinergic side effects such as dry mouth and drowsiness occurred more frequently among nortriptyline-treated patients; however, this finding was not statistically significant.55 It should be noted that this study enrolled a relatively small sample; further research is therefore warranted. Nortriptyline may be an alternative for patients in whom conventional smoking cessation therapy has failed or for patients who are not candidates for conventional smoking cessation therapy.
CONCLUSION

When making formulary decisions for smoking cessation therapy, multiple factors should be taken into account. These may include cost of therapy, patient population, adverse-effect profile, and efficacy. Each healthcare facility has differing needs based on its patient demographic. For example, an acute care facility may prefer to have various formulations of NRT on formulary rather than bupropion or varenicline given the onset of action of each therapy, whereas an outpatient smoking cessation clinic may benefit from having all options available.
Dr Wise and Dr Correia are clinical pharmacy specialists for the VA Boston Healthcare System, West Roxbury, Massachusetts, and adjunct faculty members for pharmacy practice, Massachusetts College of Pharmacy and Health Sciences, Boston.
Disclosure Information: The authors report no financial disclosures as related to products discussed in this article.
REFERENCES
1. Rosamond W, Flegal K, Furie K, et al; for the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2008 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–e146.
2. Smoking 101 fact sheet. American Lung Association website. http://www.lungusa.org/site/pp.asp?c=dvluk9o0e&b=39853. Published May 2007. Accessed January 24, 2008.
3. American Cancer Society.Cancer Facts and Figures 2007. Atlanta, GA: American Cancer Society; 2007.
4. Taylor P. Agents acting at the neuromuscular junction and autonomic ganglia. In: Hardman JG, Limbird LE, Gilman AG, eds. Goodman & Gilman's The Pharmacological Basis of Therapeutics. 10th ed. New York, NY: McGraw-Hill; 2001.
5. Le Houezec J. Role of nicotine pharmacokinetics in nicotine addiction and nicotine replacement therapy: A review. Int J Tuberc Lung Dis. 1003;7: 811–819.
6. Doering P. Substance-related disorders: Alcohol, nicotine, and caffeine. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, eds. Pharmacotherapy: A Pathophysiologic Approach. 5th ed. New York, NY: McGraw-Hill; 2002.
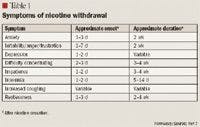
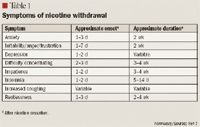
7. Hughes JR. Effects of abstinence from tobacco: Valid symptoms and time course. Nicotine Tob Res. 2007;9:315–327.
8. Kroon LA. Drug interactions with smoking. Am J Health Syst Pharm. 2007;64:1971–1921.
9. Schein JR. Cigarette smoking and clinically significant drug interactions. Ann Pharmacother. 1995;29:1139–1148.
10. Zevin S, Benowitz NL. Drug interactions with tobacco smoking. An update. Clin Pharmacokinet. 1999;36:425–438.
11. Dawson GW, Vestal RE. Smoking and drug metabolism. Pharmacol Ther. 1912;15:207–221.
12. Jenne H, Nagasawa H, McHugh R, MacDonald F, Wyse E. Decreased theophylline half-life in cigarette smokers. Life Sci. 1975;17:195–198.
13. Hunt SN, Jusko WJ, Yurchak AM. Effect of smoking on theophylline disposition. Clin Pharmacol Ther. 1976;19(5 pt 1):546–551.
14. Powell JR, Thiercelin JF, Vozeh S, Sansom L, Riegelman S. The influence of cigarette smoking and sex on theophylline disposition. Am Rev Respir Dis. 1977;116:17–23.
15. Welty D, Pool W, Woolf T, Posvan E, Sedman A. The effect of smoking on the pharmacokinetics and metabolism of cognex in healthy volunteers [abstract]. Pharm Res. 1993;10(suppl):S334.
16. Cognex [package insert]. Roswell, GA: First Horizon Pharmaceutical Corp; 2002.
17. Methiesen ER, Soegaard U, Christiansen JS. Smoking and glycaemic control in male insulin-dependent (type 1) diabetics. Diabetes Res. 1984:1; 155–157.
18. Vestal RE, Wood AJ. Influence of age and smoking on drug kinetics in man: Studies using model compounds. Clin Pharmacokinet. 1980:5:309–319.
19. Clinical depression of the central nervous system due to diazepam and chlordiazepoxide in relation to cigarette smoking and age. N Engl J Med. 1973; 288:277–280.
20. Murdock HR, Robillard NF. Use of smokers in bioavailability studies. Clin Pharmacol Ther. 1979;24:23.
21. Guide to quitting smoking. American Cancer Society website. http://www.cancer.org/docroot/ped/content/ped-10_13X_guide_for_ quitting_ smoking.asp. Accessed January 24, 2008.
22. Cigarette tax increases vs. cigarette company price increases. Campaign for Tobacco-Free Kids website. http://www.tobaccofreekids.org/research/factsheets/pdf/0210.pdf. Accessed January 30, 2008.
23. State of Tobacco Control 2006. American Lung Association website. http://lungaction.org/reports/overview06.html. Accessed January 24, 2008.
24. Sackey JA. Behavioral approach to smoking cessation. In: UpToDate. Waltham, MA; 2007.
25. A clinical practice guidelines for treating tobacco use and dependence: A US Public Health Service report. The Tobacco Use and Dependence Clinical Practice Guideline Panel, Staff, and Consortium Representatives. JAMA. 2000;283:3244–3254.
26. Practice guideline for the treatment of patients with nicotine dependence. American Psychiatric Association. Am J Psychiatry. 1996;153(10 suppl):1–31.
27. Zhu SH, Anderson C, Tedeschi GJ, et al. Evidence of real-world effectiveness of a telephone quitline for smokers. N Engl J Med. 2002;347:1087–1093.
28. Abbott N, Stead L, White A. Hypnotherapy for smoking cessation. Cochrane Database Syst Rev. 1998;(2);CD001008.
29. He D, Medbo JI, Hostmark AT. Effect of acupuncture on smoking cessation or reduction: An 8-month and 5-year follow-up study. Prev Med. 2001; 33:364–372.
30. White A, Rampes H, Ernst E. Acupuncture for smoking cessation. Cochrane Database Syst Rev. 2002;(2);CD000009.
31. NicoDerm CQ [package insert]. Moon Township, PA: GlaxoSmithKline Consumer Healthcare LP; 2006.
32. Nicorette [package insert]. Moon Township, PA: GlaxoSmithKline Consumer Healthcare LP; 2007.
33. Commit [package insert]. Moon Township, PA: GlaxoSmithKline Consumer Healthcare LP; 2006.
34. Nicotrol Inhaler [package insert]. Morris Plains, NJ: Pfizer Consumer Healthcare; 2005.
35. Nicotrol NS [package insert]. Morris Plains, NJ: Pfizer Consumer Healthcare; 2005.
36. Hajek P, West R, Foulds J, Nilsson F, Burrows S, Meadow A. Randomized comparative trial of nicotine polacrilex, a transdermal patch, nasal spray, and an inhaler. Arch Intern Med. 1999;159: 2033–2038.
37. Zyban [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2007.
38. Hurt RD, Sachs DP, Glover ED, et al. A comparison of sustained-release bupropion and placebo for smoking cessation. N Engl J Med. 1997;337: 1195–1202.
39. Hughes JR, Goldstein MG, Hurt RD, Shiffman S. Recent advances in the pharmacotherapy of smoking. JAMA. 1999;281;72–76.
40. Hays JT, Hurt RD, Rigotti NA, et al. Sustained-release bupropion for pharmacologic relapse prevention after smoking cessation: A randomized, controlled trial. Ann Intern Med. 2001;135:423–433.
41. Jorenby DE, Leischow SJ, Nides MA, et al. A controlled trial of sustained-release bupropion, a nicotine patch, or both for smoking cessation. N Engl J Med. 1999;340:685–691.
42. Potts LA, Garwood CL. Varenicline: The newest agent for smoking cessation. Am J Health Syst Pharm. 2007;64:1381–1384.
43. Etter JF. Cytisine for smoking cessation: A literature review and meta-analysis. Arch Intern Med. 2006;166:1553–1559.
44. Tutka P, Zatonski W. Cytisine for the treatment of nicotine addiction: From a molecule to therapeutic efficacy. Pharmacol Rep. 2006;58:777–798.
45. Coe JW, Brooks PR, Vetelino MG, et al. Varenicline: An alpha4beta2 nicotinic receptor partial agonist for smoking cessation. J Med Chem. 2005; 48:3474–3477.
46. Nides M, Oncken C, Gonzales D, et al. Smoking cessation with varenicline, a selective alpha4beta2 nicotinic receptor partial agonist: Results from a 7-week, randomized, placebo- and bupropion-controlled trial with 1-year follow-up. Arch Intern Med. 2006;166:1561–1568.
47. Chantix [package insert]. New York, NY: Pfizer Labs; 2008.
48. Jorenby DE, Hays JT, Rigotti NA, et al; Varenicline Phase 3 Study Group. Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: A randomized controlled trial [erratum in JAMA. 2006;296:1355]. JAMA. 2006;296:56–63.
49. Tonstad S, Tonnesen P, Hajek P, Williams KE, Billing CB, Reeves KR; Varenicline Phase 3 Study Group. Effect of maintenance therapy with varenicline on smoking cessation: A randomized controlled trial. JAMA. 2006;296:64–71.
50. Gonzales D, Rennard SI, Nides M, et al; Varenicline Phase 3 Study Group. Varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: A randomized controlled trial. JAMA. 2006;296:47–55.
51. Whitley HP, Moorman KL. Interference with smoking-cessation effects of varenicline after administration of immediate-release amphetamine-dextroamphetamine. Pharmacotherapy. 2007;27: 1440–1445.
52. Early communication about an ongoing safety review: Varenicline (marketed as Chantix). FDA website. http://www.fda.gov/cder/drug/early_comm/varenicline.htm. Accessed January 30, 2008.
53. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. 2004;(3);CD000058.
54. Prochazka AV, Kick S, Steinbrunn C, Miyoshi T, Fryer GE. A randomized trial of nortriptyline combined with transdermal nicotine for smoking cessation. Arch Intern Med. 2004;164:2229–2233.
55. da Costa CL, Younes RN, Lourenco MT. Stopping smoking: A prospective, randomized, double-blind study comparing nortriptyline to placebo. Chest. 2002;122:403–408.
56. Kaper J, Wagena EJ, Severens JL, Van Schayck CP. Healthcare financing systems for increasing the use of tobacco dependence treatment. Cochrane Database Syst Rev. 2005;(1);CD004305.
57. Mckesson supply website. http://www.supplymckesson.com/. Accessed January 30, 2008.

Employers Face Barriers With Adopting Biosimilars
March 1st 2022Despite the promise of savings billions of dollars in the United States, adoption of biosimilars has been slow. A roundtable discussion among employers highlighted some of the barriers, including formulary design and drug pricing and rebates.






